

Role of Combination Antiplatelet and Anticoagulation Therapy in Diabetes Mellitus and Cardiovascular Disease: Insights From the COMPASS Trial
- PMID: 32223318
- PMCID: PMC7314494
- DOI: 10.1161/CIRCULATIONAHA.120.046448
Role of Combination Antiplatelet and Anticoagulation Therapy in Diabetes Mellitus and Cardiovascular Disease: Insights From the COMPASS Trial
Abstract
Background: Patients with established coronary artery disease or peripheral artery disease often have diabetes mellitus. These patients are at high risk of future vascular events.
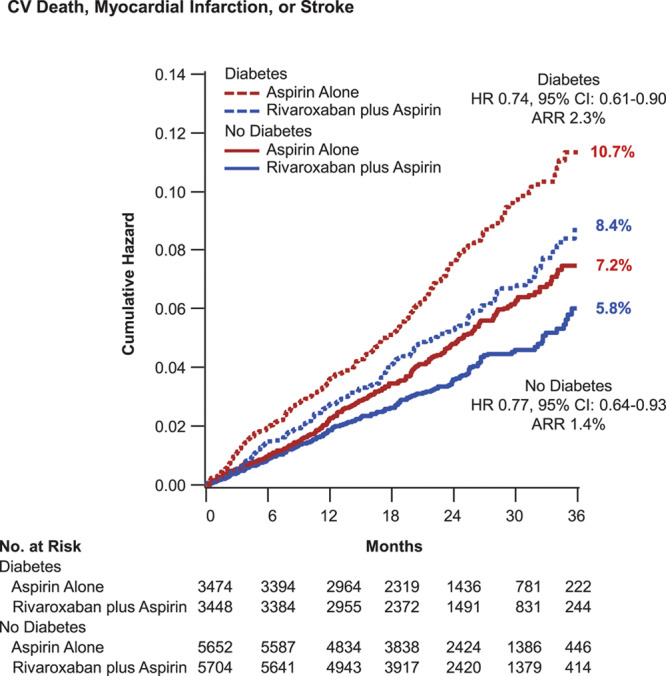
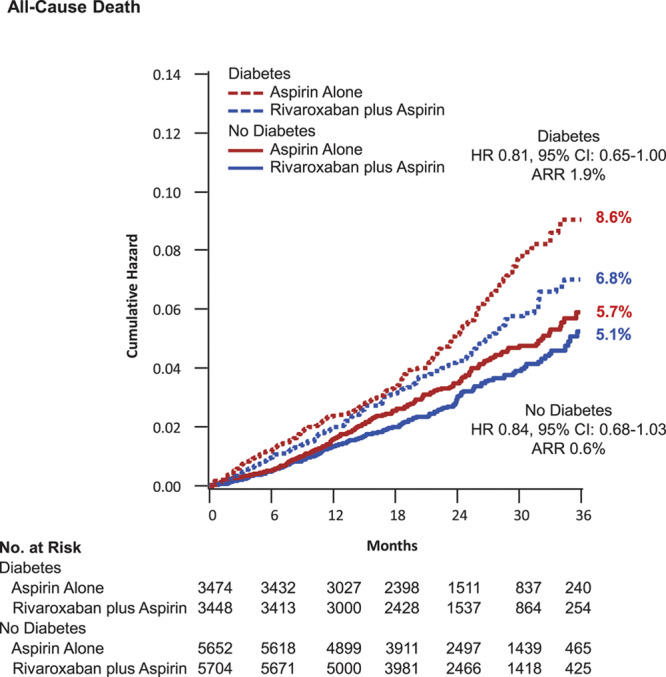
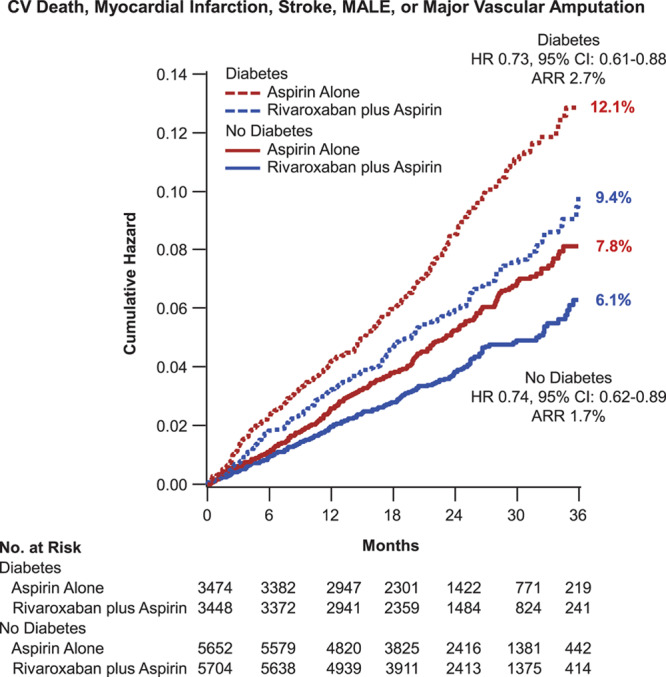
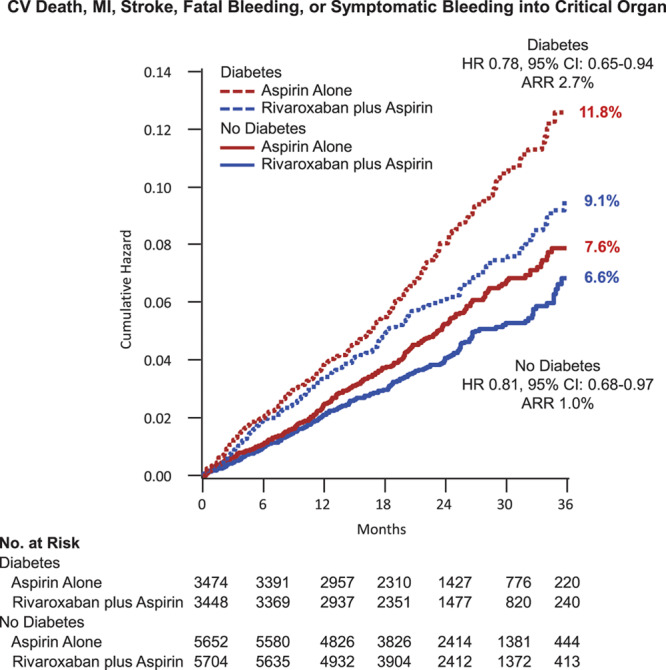
Methods: In a prespecified analysis of the COMPASS trial (Cardiovascular Outcomes for People Using Anticoagulation Strategies), we compared the effects of rivaroxaban (2.5 mg twice daily) plus aspirin (100 mg daily) versus placebo plus aspirin in patients with diabetes mellitus versus without diabetes mellitus in preventing major vascular events. The primary efficacy end point was the composite of cardiovascular death, myocardial infarction, or stroke. Secondary end points included all-cause mortality and all major vascular events (cardiovascular death, myocardial infarction, stroke, or major adverse limb events, including amputation). The primary safety end point was a modification of the International Society on Thrombosis and Haemostasis criteria for major bleeding.
Results: There were 10 341 patients with diabetes mellitus and 17 054 without diabetes mellitus in the overall trial. A consistent and similar relative risk reduction was seen for benefit of rivaroxaban plus aspirin (n=9152) versus placebo plus aspirin (n=9126) in patients both with (n=6922) and without (n=11 356) diabetes mellitus for the primary efficacy end point (hazard ratio, 0.74, P=0.002; and hazard ratio, 0.77, P=0.005, respectively, Pinteraction=0.77) and all-cause mortality (hazard ratio, 0.81, P=0.05; and hazard ratio, 0.84, P=0.09, respectively; Pinteraction=0.82). However, although the absolute risk reductions appeared numerically larger in patients with versus without diabetes mellitus, both subgroups derived similar benefit (2.3% versus 1.4% for the primary efficacy end point at 3 years, Gail-Simon qualitative Pinteraction<0.0001; 1.9% versus 0.6% for all-cause mortality, Pinteraction=0.02; 2.7% versus 1.7% for major vascular events, Pinteraction<0.0001). Because the bleeding hazards were similar among patients with and without diabetes mellitus, the prespecified net benefit for rivaroxaban appeared particularly favorable in the patients with diabetes mellitus (2.7% versus 1.0%; Gail-Simon qualitative Pinteraction=0.001).
Conclusions: In stable atherosclerosis, the combination of aspirin plus rivaroxaban 2.5 mg twice daily provided a similar relative degree of benefit on coronary, cerebrovascular, and peripheral end points in patients with and without diabetes mellitus. Given their higher baseline risk, the absolute benefits appeared larger in those with diabetes mellitus, including a 3-fold greater reduction in all-cause mortality. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT01776424.
Keywords: anticoagulants; coronary artery disease; diabetes mellitus; peripheral artery disease; platelet aggregation inhibitors.
Figures
Comment in
-
Combining Anticoagulant and Antiplatelet Therapies for Chronic Atherosclerotic Disease: A Focus on Diabetes Mellitus as a High-Risk Patient Group.Circulation. 2020 Jun 9;141(23):1855-1858. doi: 10.1161/CIRCULATIONAHA.120.046905. Epub 2020 Jun 8. Circulation. 2020. PMID: 32510996 No abstract available.
References
-
- Bhatt DL, Steg PG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, Goto S, Liau CS, Richard AJ, Röther J, et al. REACH Registry Investigators. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295:180–189. doi: 10.1001/jama.295.2.180. - PubMed
-
- Steg PG, Bhatt DL, Wilson PW, D’Agostino R, Sr, Ohman EM, Röther J, Liau CS, Hirsch AT, Mas JL, Ikeda Y, et al. REACH Registry Investigators. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA. 2007;297:1197–1206. doi: 10.1001/jama.297.11.1197. - PubMed
-
- Bhatt DL, Eagle KA, Ohman EM, Hirsch AT, Goto S, Mahoney EM, Wilson PW, Alberts MJ, D’Agostino R, Liau CS, et al. REACH Registry Investigators. Comparative determinants of 4-year cardiovascular event rates in stable outpatients at risk of or with atherothrombosis. JAMA. 2010;304:1350–1357. doi: 10.1001/jama.2010.1322. - PubMed
-
- Cavender MA, Steg PG, Smith SC, Jr, Eagle K, Ohman EM, Goto S, Kuder J, Im K, Wilson PW, Bhatt DL REACH Registry Investigators. Impact of diabetes mellitus on hospitalization for heart failure, cardiovascular events, and death: outcomes at 4 years from the Reduction of Atherothrombosis for Continued Health (REACH) Registry. Circulation. 2015;132:923–931. doi: 10.1161/CIRCULATIONAHA.114.014796. - PubMed
-
- Alberts MJ, Bhatt DL, Mas JL, Ohman EM, Hirsch AT, Röther J, Salette G, Goto S, Smith SC, Jr, Liau CS, et al. REduction of Atherothrombosis for Continued Health Registry Investigators. Three-year follow-up and event rates in the international REduction of Atherothrombosis for Continued Health Registry. Eur Heart J. 2009;30:2318–2326. doi: 10.1093/eurheartj/ehp355. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
