

Factors associated with the prescribing of high-dose opioids in primary care: a systematic review and meta-analysis
- PMID: 32223746
- PMCID: PMC7104520
- DOI: 10.1186/s12916-020-01528-7
Factors associated with the prescribing of high-dose opioids in primary care: a systematic review and meta-analysis
Abstract
Background: The risks of harms from opioids increase substantially at high doses, and high-dose prescribing has increased in primary care. However, little is known about what leads to high-dose prescribing, and studies exploring this have not been synthesized. We, therefore, systematically synthesized factors associated with the prescribing of high-dose opioids in primary care.
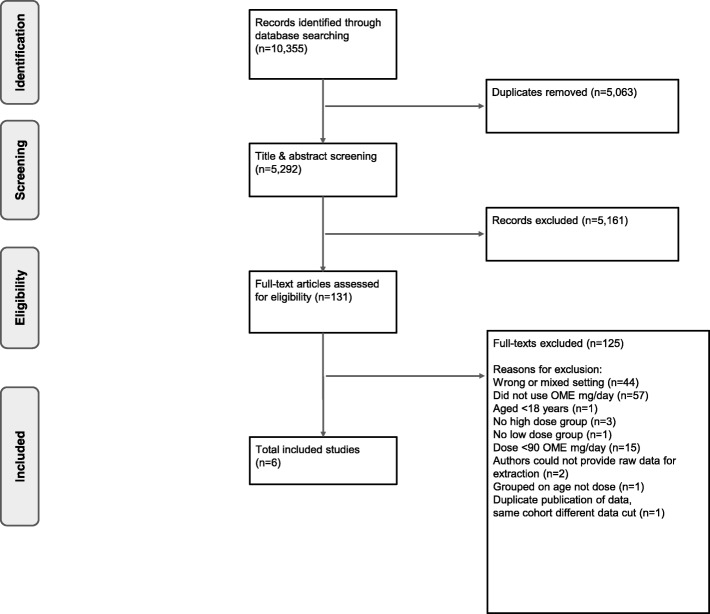
Methods: We conducted a systematic review of observational studies in high-income countries that used patient-level primary care data and explored any factor(s) in people for whom opioids were prescribed, stratified by oral morphine equivalents (OME). We defined high doses as ≥ 90 OME mg/day. We searched MEDLINE, Embase, Web of Science, reference lists, forward citations, and conference proceedings from database inception to 5 April 2019. Two investigators independently screened studies, extracted data, and appraised the quality of included studies using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. We pooled data on factors using random effects meta-analyses and reported relative risks (RR) or mean differences with 95% confidence intervals (CI) where appropriate. We also performed a number needed to harm (NNTH) calculation on factors when applicable.
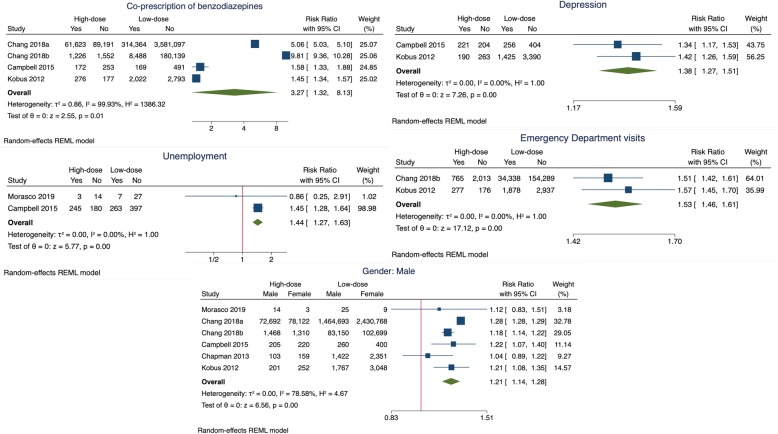
Results: We included six studies with a total of 4,248,119 participants taking opioids, of whom 3.64% (n = 154,749) were taking high doses. The majority of included studies (n = 4) were conducted in the USA, one in Australia and one in the UK. The largest study (n = 4,046,275) was from the USA. Included studies were graded as having fair to good quality evidence. The co-prescription of benzodiazepines (RR 3.27, 95% CI 1.32 to 8.13, I2 = 99.9%), depression (RR 1.38, 95% CI 1.27 to 1.51, I2 = 0%), emergency department visits (RR 1.53, 95% CI 1.46 to 1.61, I2 = 0%, NNTH 15, 95% CI 12 to 20), unemployment (RR 1.44, 95% CI 1.27 to 1.63, I2 = 0%), and male gender (RR 1.21, 95% CI 1.14 to 1.28, I2 = 78.6%) were significantly associated with the prescribing of high-dose opioids in primary care.
Conclusions: High doses of opioids are associated with greater risks of harms. Associated factors such as the co-prescription of benzodiazepines and depression identify priority areas that should be considered when selecting, identifying, and managing people taking high-dose opioids in primary care. Coordinated strategies and services that promote the safe prescribing of opioids are needed.
Study registration: PROSPERO, CRD42018088057.
Keywords: Benzodiazepines; Depression; Emergency department; High dose; Opioids; Primary care; Systematic review.
Conflict of interest statement
GCR is funded by the NIHR SPCR Research Doctoral Studentship, the Naji Foundation, and the Rotary Foundation. KRM has received funding from NIHR and the Royal College of General Practitioners (RCGP) to conduct independent research. TBM is financially supported by the Rhodes Trust to study for a Doctor of Philosophy. NJD is employed on BG’s grants from the Laura and John Arnold Foundation and is financially supported by the Naji Foundation to study for a Doctor of Philosophy. CK is funded by the NIHR SPCR and the Wellcome Trust/Royall Society Sir Henry Dale Fellowship. JKA has written papers on adverse drug reactions in peer-reviewed journals and has received royalties from textbooks that he has edited or co-edited. JKA has often acted as an expert witness in cases involving adverse drug reactions, most often in Coroners’ courts. BG receives funding from the Health Foundation, the NIHR SPCR, the NIHR Biomedical Research Centre Oxford, and the NHS England for work on UK prescribing data. BG has additionally received funding from the Laura and John Arnold Foundation, the Wellcome Trust, and WHO to work on better use of data in medicine and receives personal income from speaking and writing for lay audiences on the misuse of science. CJH has received funding from the WHO, FDA, NIHR, NIHR SPCR, and NIHR BRC Oxford; received expenses and fees for his media work (including payments from BBC Radio 4 Inside Health), remuneration from an asbestos case and given free legal advice on mesh cases, income from the publication of a series of toolkit books published by Blackwells, and expenses for teaching EBM; and is also paid for his GP work in NHS out of hours (contract with Oxford Health NHS Foundation Trust). CJH is the Director of CEBM, which jointly runs the EvidenceLive Conference with the BMJ and the Overdiagnosis Conference with international partners, based on a non-profit making model. CJH is the Editor in Chief of BMJ Evidence-Based Medicine and is an NIHR Senior Investigator.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
