

Comparison of Hospitalized Patients With ARDS Caused by COVID-19 and H1N1
- PMID: 32224074
- PMCID: PMC7151343
- DOI: 10.1016/j.chest.2020.03.032
Comparison of Hospitalized Patients With ARDS Caused by COVID-19 and H1N1
Abstract
Background: Since the outbreak of coronavirus disease 2019 (COVID-19) in China in December 2019, considerable attention has been focused on its elucidation. However, it is also important for clinicians and epidemiologists to differentiate COVID-19 from other respiratory infectious diseases such as influenza viruses.
Research question: The aim of this study was to explore the different clinical presentations between COVID-19 and influenza A (H1N1) pneumonia in patients with ARDS.
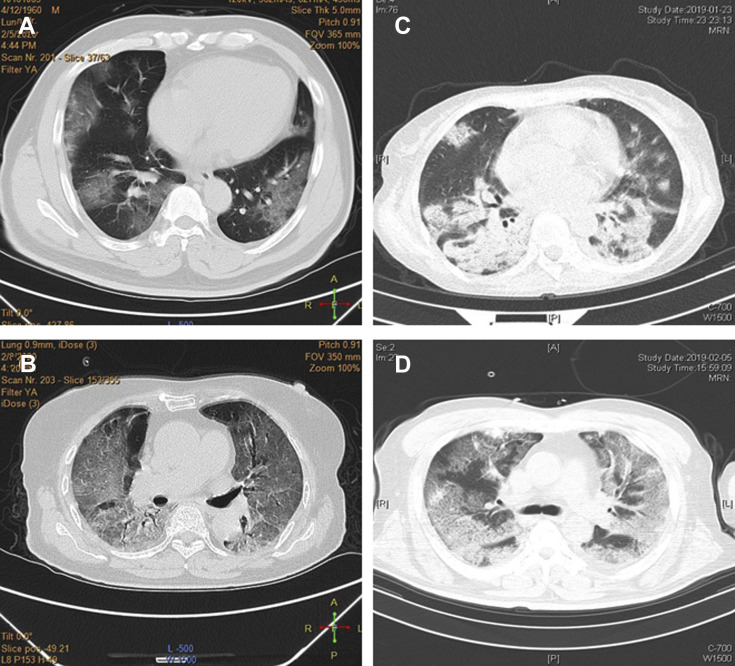
Study design and methods: This analysis was a retrospective case-control study. Two independent cohorts of patients with ARDS infected with either COVID-19 (n = 73) or H1N1 (n = 75) were compared. Their clinical manifestations, imaging characteristics, treatments, and prognosis were analyzed and compared.
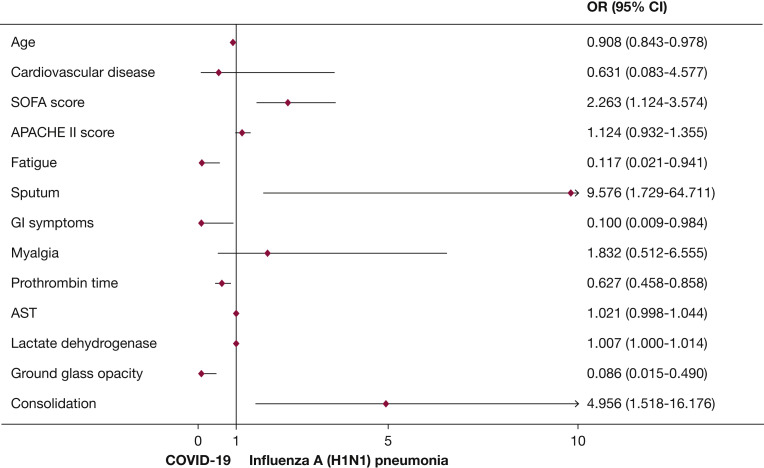
Results: The median age of patients with COVID-19 was higher than that of patients with H1N1, and there was a higher proportion of male subjects among the H1N1 cohort (P < .05). Patients with COVID-19 exhibited higher proportions of nonproductive coughs, fatigue, and GI symptoms than those of patients with H1N1 (P < .05). Patients with H1N1 had higher Sequential Organ Failure Assessment (SOFA) scores than patients with COVID-19 (P < .05). The Pao2/Fio2 of 198.5 mm Hg in the COVID-19 cohort was significantly higher than the Pao2/Fio2 of 107.0 mm Hg in the H1N1 cohort (P < .001). Ground-glass opacities was more common in patients with COVID-19 than in patients with H1N1 (P < .001). There was a greater variety of antiviral therapies administered to COVID-19 patients than to H1N1 patients. The in-hospital mortality of patients with COVID-19 was 28.8%, whereas that of patients with H1N1 was 34.7% (P = .483). SOFA score-adjusted mortality of H1N1 patients was significantly higher than that of COVID-19 patients, with a rate ratio of 2.009 (95% CI, 1.563-2.583; P < .001).
Interpretation: There were many differences in clinical presentations between patients with ARDS infected with either COVID-19 or H1N1. Compared with H1N1 patients, patients with COVID-19-induced ARDS had lower severity of illness scores at presentation and lower SOFA score-adjusted mortality.
Keywords: ARDS; COVID-19; H1N1; influenza A; mortality.
Copyright © 2020. Published by Elsevier Inc.
Figures
References
-
- World Health Organization Coronavirus disease (COVID-2019) situation reports-50. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
