

Imaging of Emerging Infectious Diseases
- PMID: 32226652
- PMCID: PMC7100865
- DOI: 10.1007/s40134-019-0338-4
Imaging of Emerging Infectious Diseases
Abstract
Purpose of review: Emerging infectious diseases have seen a record increase in prevalence, and understanding their management is critical in an increasingly global community. In this paper, we review current literature detailing the role of radiology in the diagnosis and treatment of the Ebola (EVD), Zika (ZVD), Chikungunya (CHIKF), H1N1, Middle East Respiratory (MERS), and Severe Acute Respiratory Syndrome (SARS) viruses.
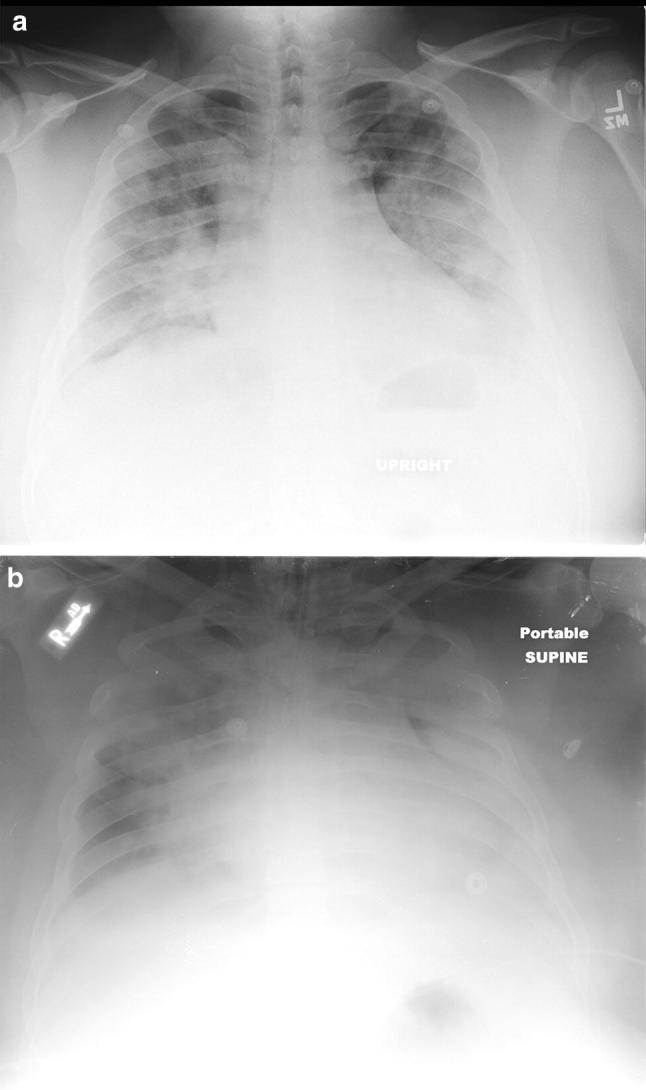
Recent findings: Complex protocols are required to safely use portable imaging in EVD to prevent nosocomial spread of disease. In ZVD, antenatal ultrasound can detect fetal abnormalities early, allowing implementation of care and support to affected families. Imaging is useful in assessing the extent of involvement of chronic CHIKF and monitoring treatment effect. Chest radiography and CT play a more direct role in the diagnosis and monitoring of the viral infections with primarily respiratory manifestations (H1N1, MERS, and SARS).
Summary: Radiology plays a variable role in emerging infectious diseases, requiring an understanding of disease transmission and safe imaging practices, as well as imaging features that affect clinical management.
Keywords: Chikungunya; Ebola; Emerging disease; H1N1; MERS; SARS; Zika.
© Springer Science+Business Media, LLC, part of Springer Nature 2019.
Conflict of interest statement
Conflict of interestAll the authors declared that they have no potential conflicts of interest.
Figures









References
-
- World Health Organization. The World Health Report 2007: a safer future: global public health security in the 21st century, 2007, ISBN 978 92 4 156344 4. https://www.who.int/whr/2007/en/. Accessed 1 Feb 2019.
-
- The National Institute for Occupational Safety and Health. Emerging Infectious Diseases, 2018, Centers for Disease Control, https://www.cdc.gov/niosh/topics/emerginfectdiseases/default.html. Accessed 1 Feb 2019.
-
- World Health Organization. Ebola Virus Disease, 2018. https://www.who.int/news-room/fact-sheets/detail/ebola-virus-disease. Accessed 1 Feb 2019.
-
- Centers for Disease Control. Ebola in Democratic Republic of the Congo, 2018. http://wwwnc.cdc.gov/trave/notices/alert/ebola-democratic-republic-of-th.... Accessed 1 Feb 2019.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous