

Comparison of the Effectiveness of Single-Component and Multicomponent Interventions for Reducing Radiation Doses in Patients Undergoing Computed Tomography: A Randomized Clinical Trial
- PMID: 32227142
- PMCID: PMC7105953
- DOI: 10.1001/jamainternmed.2020.0064
Comparison of the Effectiveness of Single-Component and Multicomponent Interventions for Reducing Radiation Doses in Patients Undergoing Computed Tomography: A Randomized Clinical Trial
Abstract
Importance: Computed tomography (CT) radiation doses vary across institutions and are often higher than needed.
Objective: To assess the effectiveness of 2 interventions to reduce radiation doses in patients undergoing CT.
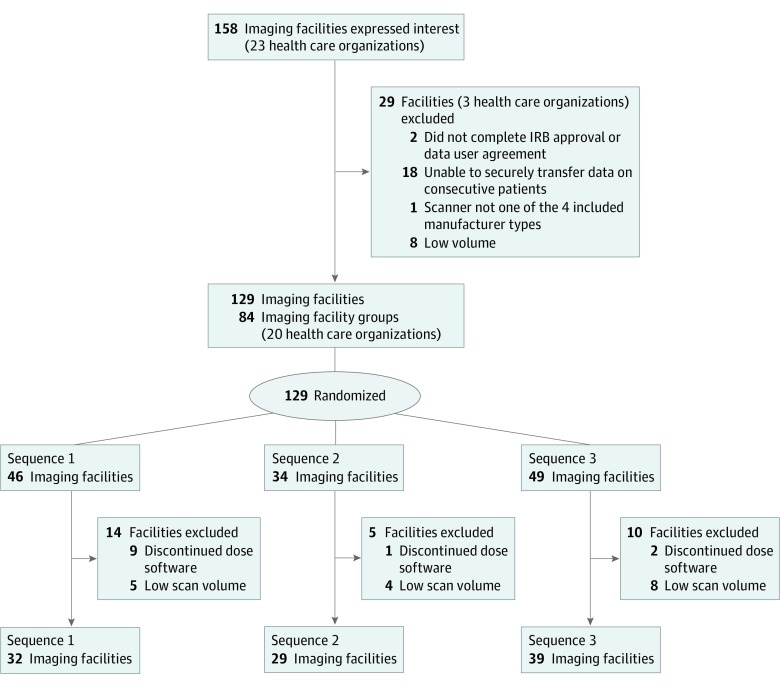
Design, setting, and participants: This randomized clinical trial included 864 080 adults older than 18 years who underwent CT of the abdomen, chest, combined abdomen and chest, or head at 100 facilities in 6 countries from November 1, 2015, to September 21, 2017. Data analysis was performed from October 4, 2017, to December 14, 2018.
Interventions: Imaging facilities received audit feedback alone comparing radiation-dose metrics with those of other facilities followed by the multicomponent intervention, including audit feedback with targeted suggestions, a 7-week quality improvement collaborative, and best-practice sharing. Facilities were randomly allocated to the time crossing from usual care to the intervention.
Main outcomes and measures: Primary outcomes were the proportion of high-dose CT scans and mean effective dose at the facility level. Secondary outcomes were organ doses. Outcomes after interventions were compared with those before interventions using hierarchical generalized linear models adjusting for temporal trends and patient characteristics.
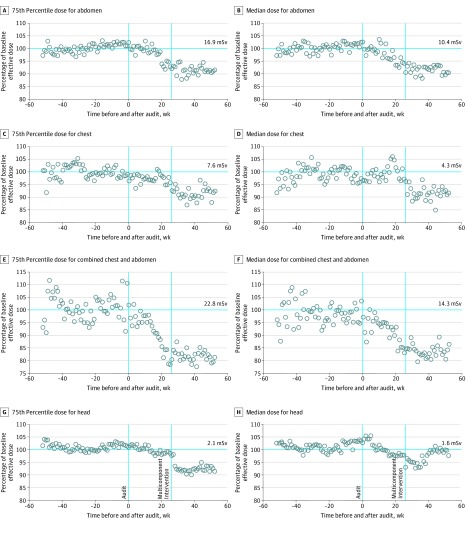
Results: Across 100 facilities, 864 080 adults underwent 1 156 657 CT scans. The multicomponent intervention significantly reduced proportions of high-dose CT scans, measured using effective dose. Absolute changes in proportions of high-dose scans were 1.1% to 7.9%, with percentage reductions in the proportion of high-dose scans of 4% to 30% (abdomen: odds ratio [OR], 0.82; 95% CI, 0.77-0.88; P < .001; chest: OR, 0.92; 95% CI, 0.86-0.99; P = .03; combined abdomen and chest: OR, 0.49; 95% CI, 0.41-0.59; P < .001; and head: OR, 0.71; 95% CI, 0.66-0.76; P < .001). Reductions in the proportions of high-dose scans were greater when measured using organ doses. The absolute reduction in the proportion of high-dose scans was 6.0% to 17.2%, reflecting 23% to 58% reductions in the proportions of high-dose scans across anatomical areas. Mean effective doses were significantly reduced after multicomponent intervention for abdomen (6% reduction, P < .001), chest (4%, P < .001), and chest and abdomen (14%, P < .001) CT scans. Larger reductions in mean organ doses were 8% to 43% across anatomical areas. Audit feedback alone reduced the proportions of high-dose scans and mean dose, but reductions in observed dose were smaller. Radiologist's satisfaction with CT image quality was unchanged and high during all periods.
Conclusions and relevance: For imaging facilities, detailed feedback on CT radiation dose combined with actionable suggestions and quality improvement education significantly reduced doses, particularly organ doses. Effects of audit feedback alone were modest.
Trial registration: ClinicalTrials.gov Identifier: NCT03000751.
Conflict of interest statement
Figures
References
-
- National Council on Radiation Protection and Measurements Ionizing Radiation Exposure of the Population of the United States, 2009. Bethesda, MD: National Council on Radiation Protection and Measurements; 2009. NCRP report 160.
-
- Medical Radiation Exposure of the European Population: Part 1/2. Luxenbourg, Sweden: Luxenbourg Publications Office of the European Union; 2014. European Commission Medical Protection No. 180.
-
- Board of Radiation Effects Research Division on Earth and Life Sciences National Research Council of the National Academies Health Risks From Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2. Washington, DC: National Academies Press; 2006. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
