

Engineered M13 Peptide Carrier Promotes Angiogenic Potential of Patient-Derived Human Cardiac Progenitor Cells and In Vivo Engraftment
- PMID: 32227286
- PMCID: PMC7260304
- DOI: 10.1007/s13770-020-00244-w
Engineered M13 Peptide Carrier Promotes Angiogenic Potential of Patient-Derived Human Cardiac Progenitor Cells and In Vivo Engraftment
Abstract
Background: Despite promising advances in stem cell-based therapy, the treatment of ischemic cardiovascular diseases remains a big challenge due to both the insufficient in vivo viability of transplanted cells and poor angiogenic potential of stem cells. The goal of this study was to develop therapeutic human cardiac progenitor cells (hCPCs) for ischemic cardiovascular diseases with a novel M13 peptide carrier.
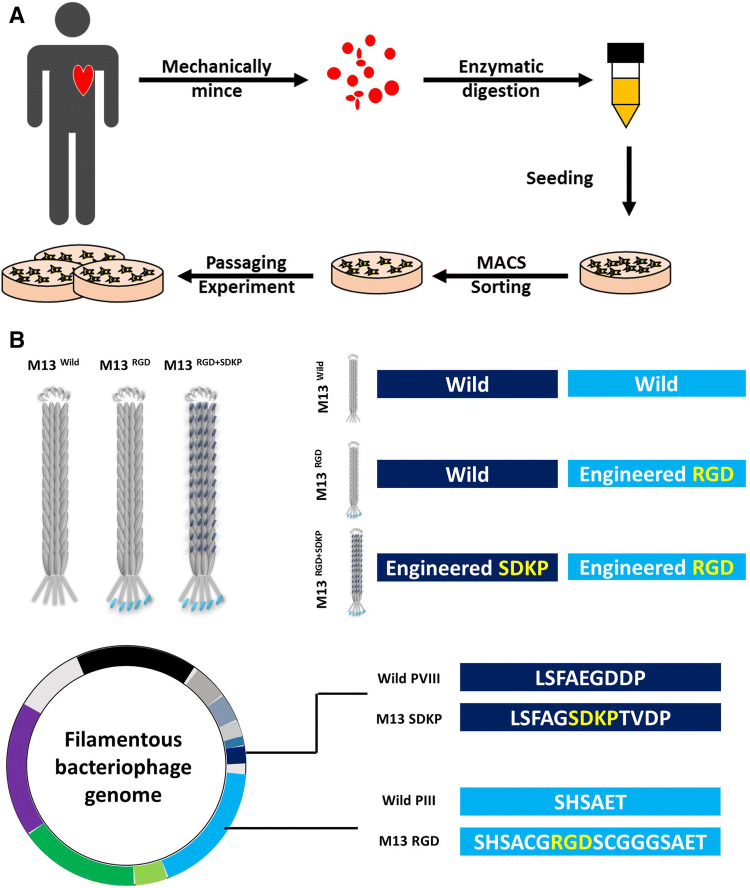
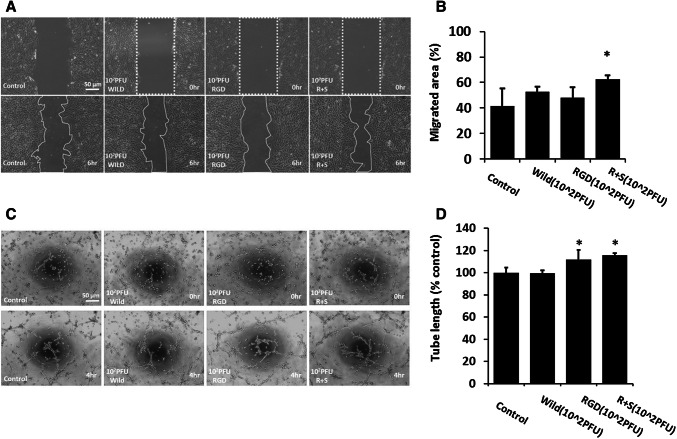
Method: In this study, an engineered M13 peptide carrier was successfully generated using a QuikChange Kit. The cellular function of M13 peptide carrier-treated hCPCs was assessed using a tube formation assay and scratch wound healing assay. The in vivo engraftment and cell survival bioactivities of transplanted cells were demonstrated by immunohistochemistry after hCPC transplantation into a myocardial infarction animal model.
Results: The engineered M13RGD+SDKP peptide carrier, which expressed RGD peptide on PIII site and SDKP peptide on PVIII site, did not affect morphologic change and proliferation ability in hCPCs. In contrast, hCPCs treated with M13RGD+SDKP showed enhanced angiogenic capacity, including tube formation and migration capacity. Moreover, transplanted hCPCs with M13RGD+SDKP were engrafted into the ischemic region and promoted in vivo cell survival.
Conclusion: Our present data provides a promising protocol for CPC-based cell therapy via short-term cell priming of hCPCs with engineered M13RGD+SDKP before cell transplantation for treatment of cardiovascular disease.
Keywords: Cardiac progenitor cell; Cardiovascular diseases; M13 bacteriophage; RGD; SDKP.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures




References
-
- Moran AE, Roth GA, Narula J, Mensah GA. 1990–2010 Global cardiovascular disease Atlas. Glob Heart. 2014;9:3–16. - PubMed
-
- Thomas H, Diamond J, Vieco A, Chaudhuri S, Shinnar E, Cromer S, et al. Global Atlas of cardiovascular disease 2000–2016: the path to prevention and control. Glob Heart. 2018;13:143–163. - PubMed
-
- De Caterina R, Zampolli A, Del Turco S, Madonna R, Massaro M. Nutritional mechanisms that influence cardiovascular disease. Am J Clin Nutr. 2006;83:421S–426S. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical