

How technology is driving the landscape of epilepsy surgery
- PMID: 32227349
- PMCID: PMC7317716
- DOI: 10.1111/epi.16489
How technology is driving the landscape of epilepsy surgery
Abstract
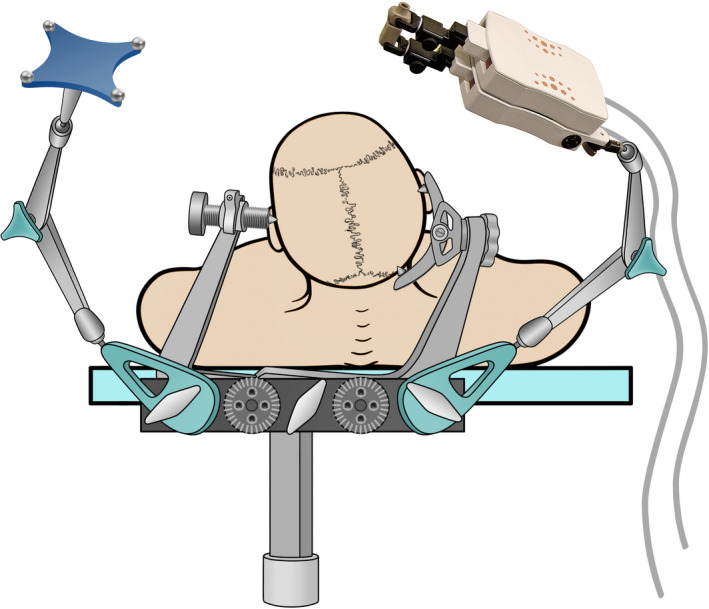
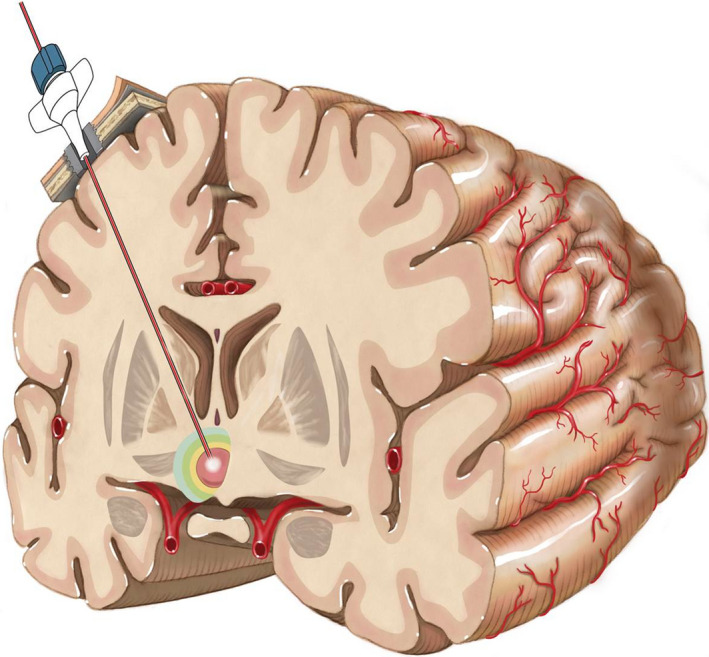
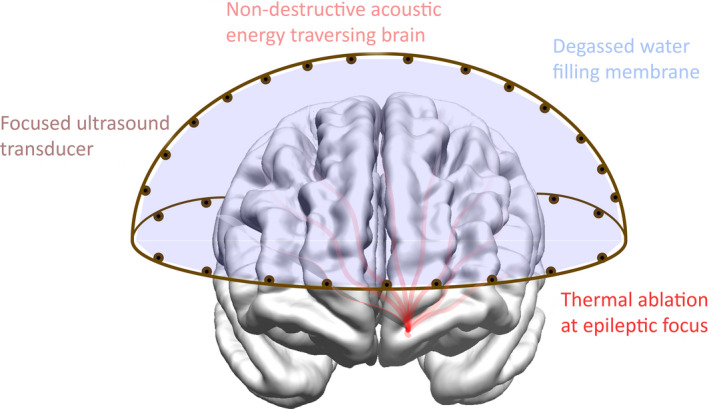
This article emphasizes the role of the technological progress in changing the landscape of epilepsy surgery and provides a critical appraisal of robotic applications, laser interstitial thermal therapy, intraoperative imaging, wireless recording, new neuromodulation techniques, and high-intensity focused ultrasound. Specifically, (a) it relativizes the current hype in using robots for stereo-electroencephalography (SEEG) to increase the accuracy of depth electrode placement and save operating time; (b) discusses the drawback of laser interstitial thermal therapy (LITT) when it comes to the need for adequate histopathologic specimen and the fact that the concept of stereotactic disconnection is not new; (c) addresses the ratio between the benefits and expenditure of using intraoperative magnetic resonance imaging (MRI), that is, the high technical and personnel expertise needed that might restrict its use to centers with a high case load, including those unrelated to epilepsy; (d) soberly reviews the advantages, disadvantages, and future potentials of neuromodulation techniques with special emphasis on the differences between closed and open-loop systems; and (e) provides a critical outlook on the clinical implications of focused ultrasound, wireless recording, and multipurpose electrodes that are already on the horizon. This outlook shows that although current ultrasonic systems do have some limitations in delivering the acoustic energy, further advance of this technique may lead to novel treatment paradigms. Furthermore, it highlights that new data streams from multipurpose electrodes and wireless transmission of intracranial recordings will become available soon once some critical developments will be achieved such as electrode fidelity, data processing and storage, heat conduction as well as rechargeable technology. A better understanding of modern epilepsy surgery will help to demystify epilepsy surgery for the patients and the treating physicians and thereby reduce the surgical treatment gap.
Keywords: epilepsy surgery; high-intensity focused ultrasound; intraoperative MRI; laser ablation; neuromodulation; robots.
© 2020 The Authors. Epilepsia published by Wiley Periodicals, Inc. on behalf of International League Against Epilepsy.
Conflict of interest statement
None of the authors has any conflict of interest to disclose. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures
References
-
- Wiebe S, Blume WT, Girvin JP, Eliasziw M. A randomized, controlled trial of surgery for temporal‐lobe epilepsy. N Engl J Med. 2001;345:311–8. - PubMed
-
- Van Gompel JJ, Worrell GA, Bell ML, Patrick TA, Cascino GD, Raffel C, et al. Intracranial electroencephalography with subdural grid electrodes: techniques, complications, and outcomes. Neurosurgery. 2008;63:498–505. - PubMed
-
- Lüders H, Awad I, Burgess R, Wyllie E, Van Ness P. Subdural electrodes in the presurgical evaluation for surgery of epilepsy. Epilepsy Res Suppl. 1992;5:147–56. - PubMed
-
- Bancaud J, Talairach J. La Stereo‐Electroencephalographie Dans L´epilepsie. Paris, France: M. CIE, 1965.
-
- Cardinale F, Cossu M, Castana L, Casaceli G, Schiariti MP, Miserocchi A, et al. Stereoelectroencephalography: surgical methodology, safety, and stereotactic application accuracy in 500 procedures. Neurosurgery. 2013;72:353–66. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
