

Health-Status Outcomes with Invasive or Conservative Care in Coronary Disease
- PMID: 32227753
- PMCID: PMC7261489
- DOI: 10.1056/NEJMoa1916370
Health-Status Outcomes with Invasive or Conservative Care in Coronary Disease
Abstract
Background: In the ISCHEMIA trial, an invasive strategy with angiographic assessment and revascularization did not reduce clinical events among patients with stable ischemic heart disease and moderate or severe ischemia. A secondary objective of the trial was to assess angina-related health status among these patients.
Methods: We assessed angina-related symptoms, function, and quality of life with the Seattle Angina Questionnaire (SAQ) at randomization, at months 1.5, 3, and 6, and every 6 months thereafter in participants who had been randomly assigned to an invasive treatment strategy (2295 participants) or a conservative strategy (2322). Mixed-effects cumulative probability models within a Bayesian framework were used to estimate differences between the treatment groups. The primary outcome of this health-status analysis was the SAQ summary score (scores range from 0 to 100, with higher scores indicating better health status). All analyses were performed in the overall population and according to baseline angina frequency.
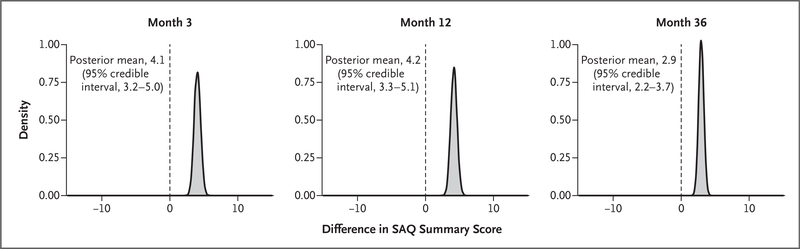
Results: At baseline, 35% of patients reported having no angina in the previous month. SAQ summary scores increased in both treatment groups, with increases at 3, 12, and 36 months that were 4.1 points (95% credible interval, 3.2 to 5.0), 4.2 points (95% credible interval, 3.3 to 5.1), and 2.9 points (95% credible interval, 2.2 to 3.7) higher with the invasive strategy than with the conservative strategy. Differences were larger among participants who had more frequent angina at baseline (8.5 vs. 0.1 points at 3 months and 5.3 vs. 1.2 points at 36 months among participants with daily or weekly angina as compared with no angina).
Conclusions: In the overall trial population with moderate or severe ischemia, which included 35% of participants without angina at baseline, patients randomly assigned to the invasive strategy had greater improvement in angina-related health status than those assigned to the conservative strategy. The modest mean differences favoring the invasive strategy in the overall group reflected minimal differences among asymptomatic patients and larger differences among patients who had had angina at baseline. (Funded by the National Heart, Lung, and Blood Institute and others; ISCHEMIA ClinicalTrials.gov number, NCT01471522.).
Copyright © 2020 Massachusetts Medical Society.
Figures


Comment in
-
Managing Stable Ischemic Heart Disease.N Engl J Med. 2020 Apr 9;382(15):1468-1470. doi: 10.1056/NEJMe2000239. Epub 2020 Mar 30. N Engl J Med. 2020. PMID: 32227752 No abstract available.
-
Initial medical therapy for moderate to severe ISCHEMIA.Nat Rev Cardiol. 2020 Jun;17(6):319. doi: 10.1038/s41569-020-0383-y. Nat Rev Cardiol. 2020. PMID: 32273612 No abstract available.
-
[Among patients with stable coronary disease and moderate or severe ischemia, does coronary angiography and revascularization when possible plus optimal medical treatment result in better clinical outcomes compared with optimal medical therapy alone?].Rev Med Interne. 2020 Jul;41(7):504-505. doi: 10.1016/j.revmed.2020.06.007. Epub 2020 Jul 14. Rev Med Interne. 2020. PMID: 32674897 French. No abstract available.
-
Invasive therapy improved angina health status in patients with high-risk stable coronary disease and more frequent angina.Ann Intern Med. 2020 Aug 18;173(4):JC15. doi: 10.7326/ACPJ202008180-015. Ann Intern Med. 2020. PMID: 32805176
-
Invasive or Conservative Strategy for Stable Coronary Disease.N Engl J Med. 2020 Sep 3;383(10):e66. doi: 10.1056/NEJMc2024008. N Engl J Med. 2020. PMID: 32877591 No abstract available.
-
Invasive or Conservative Strategy for Stable Coronary Disease.N Engl J Med. 2020 Sep 3;383(10):e66. doi: 10.1056/NEJMc2024008. N Engl J Med. 2020. PMID: 32877592 No abstract available.
-
Invasive or Conservative Strategy for Stable Coronary Disease.N Engl J Med. 2020 Sep 3;383(10):e66. doi: 10.1056/NEJMc2024008. N Engl J Med. 2020. PMID: 32877593 No abstract available.
-
Invasive or Conservative Strategy for Stable Coronary Disease.N Engl J Med. 2020 Sep 3;383(10):e66. doi: 10.1056/NEJMc2024008. N Engl J Med. 2020. PMID: 32877594 No abstract available.
-
Invasive or Conservative Strategy for Stable Coronary Disease.N Engl J Med. 2020 Sep 3;383(10):e66. doi: 10.1056/NEJMc2024008. N Engl J Med. 2020. PMID: 32877595 No abstract available.
References
-
- Smith SC Jr, Benjamin EJ, Bonow RO, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation 2011;124:2458–73. - PubMed
-
- Smith SC Jr, Allen J, Blair SN, et al. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the National Heart, Lung, and Blood Institute. Circulation 2006;113:2363–72. - PubMed
-
- Patel MR, Calhoon JH, Dehmer GJ, et al. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 appropriate use criteria for coronary revascularization in patients with stable ischemic heart disease: a report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, and Society of Thoracic Surgeons. J Am Coll Cardiol 2017;69:2212–41. - PubMed
-
- Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2012;126(25):e354–e471. - PubMed
-
- Weintraub WS, Spertus JA, Kolm P, et al. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med 2008;359:677–87. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U01 HL105561/HL/NHLBI NIH HHS/United States
- U01 HL105907/HL/NHLBI NIH HHS/United States
- U01 HL105565/HL/NHLBI NIH HHS/United States
- U01HL105462/HL/NHLBI NIH HHS/United States
- U01HL105565/HL/NHLBI NIH HHS/United States
- UL1 TR002243/TR/NCATS NIH HHS/United States
- U01HL105561/HL/NHLBI NIH HHS/United States
- UL1 TR002243/HL/NHLBI NIH HHS/United States
- UL1 TR001445/TR/NCATS NIH HHS/United States
- U01HL105907/HL/NHLBI NIH HHS/United States
- U01 HL105462/HL/NHLBI NIH HHS/United States
- U01 HL117905/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical