

Health Status after Invasive or Conservative Care in Coronary and Advanced Kidney Disease
- PMID: 32227754
- PMCID: PMC7255621
- DOI: 10.1056/NEJMoa1916374
Health Status after Invasive or Conservative Care in Coronary and Advanced Kidney Disease
Abstract
Background: In the ISCHEMIA-CKD trial, the primary analysis showed no significant difference in the risk of death or myocardial infarction with initial angiography and revascularization plus guideline-based medical therapy (invasive strategy) as compared with guideline-based medical therapy alone (conservative strategy) in participants with stable ischemic heart disease, moderate or severe ischemia, and advanced chronic kidney disease (an estimated glomerular filtration rate of <30 ml per minute per 1.73 m2 or receipt of dialysis). A secondary objective of the trial was to assess angina-related health status.
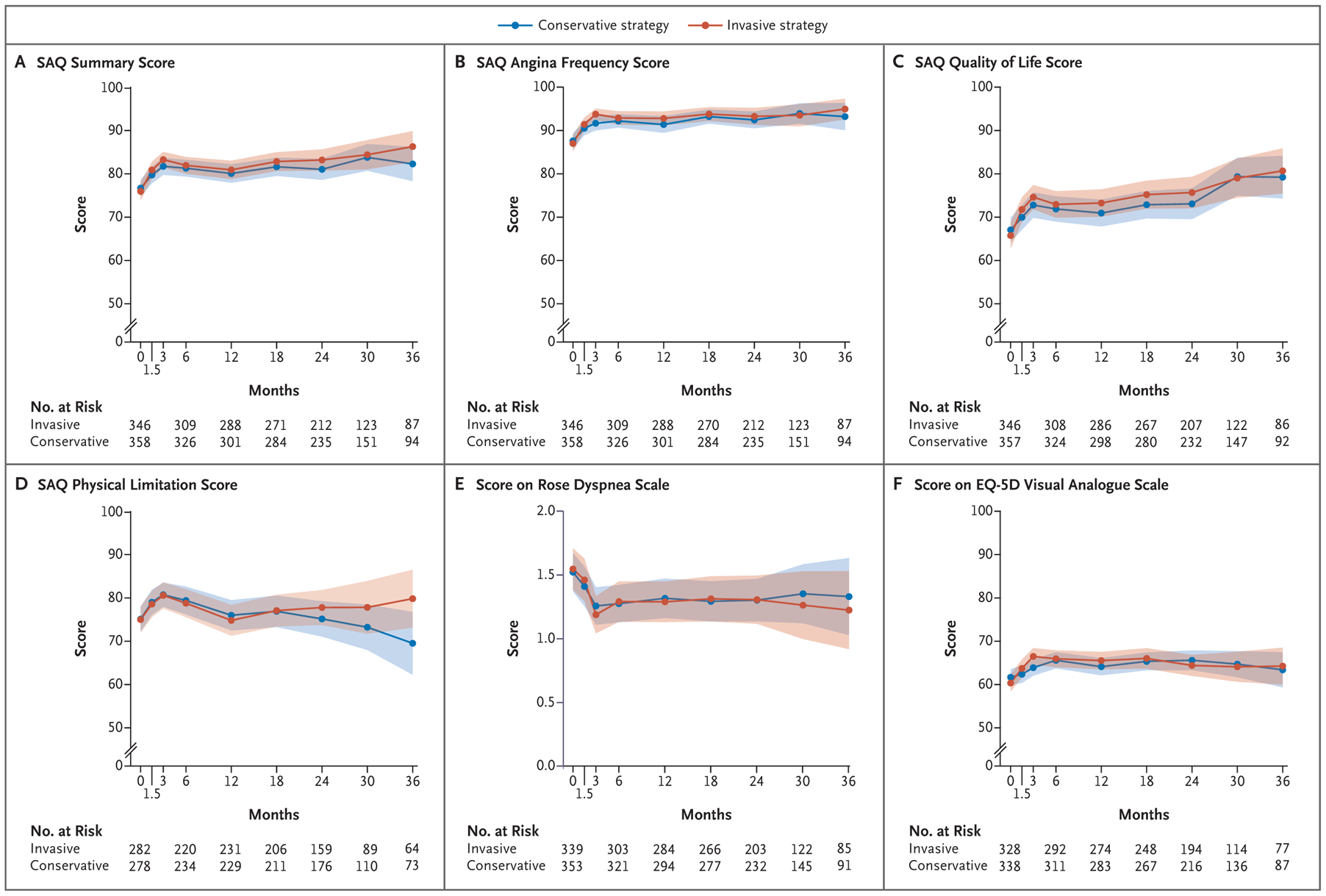
Methods: We assessed health status with the Seattle Angina Questionnaire (SAQ) before randomization and at 1.5, 3, and 6 months and every 6 months thereafter. The primary outcome of this analysis was the SAQ Summary score (ranging from 0 to 100, with higher scores indicating less frequent angina and better function and quality of life). Mixed-effects cumulative probability models within a Bayesian framework were used to estimate the treatment effect with the invasive strategy.
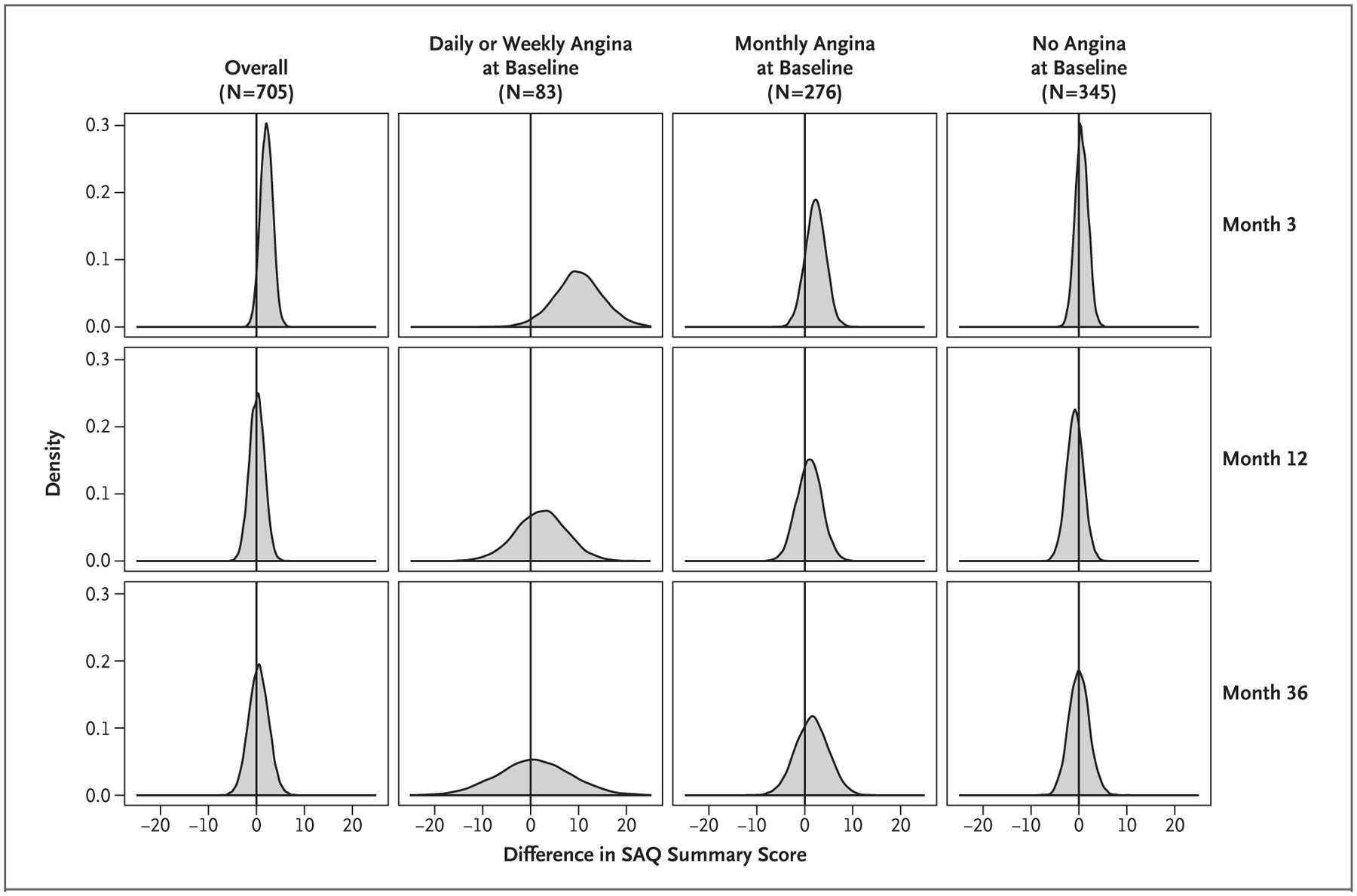
Results: Health status was assessed in 705 of 777 participants. Nearly half the participants (49%) had had no angina during the month before randomization. At 3 months, the estimated mean difference between the invasive-strategy group and the conservative-strategy group in the SAQ Summary score was 2.1 points (95% credible interval, -0.4 to 4.6), a result that favored the invasive strategy. The mean difference in score at 3 months was largest among participants with daily or weekly angina at baseline (10.1 points; 95% credible interval, 0.0 to 19.9), smaller among those with monthly angina at baseline (2.2 points; 95% credible interval, -2.0 to 6.2), and nearly absent among those without angina at baseline (0.6 points; 95% credible interval, -1.9 to 3.3). By 6 months, the between-group difference in the overall trial population was attenuated (0.5 points; 95% credible interval, -2.2 to 3.4).
Conclusions: Participants with stable ischemic heart disease, moderate or severe ischemia, and advanced chronic kidney disease did not have substantial or sustained benefits with regard to angina-related health status with an initially invasive strategy as compared with a conservative strategy. (Funded by the National Heart, Lung, and Blood Institute; ISCHEMIA-CKD ClinicalTrials.gov number, NCT01985360.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
No benefit of initial invasive strategy for managing CAD in advanced CKD.Nat Rev Cardiol. 2020 Jun;17(6):320-321. doi: 10.1038/s41569-020-0384-x. Nat Rev Cardiol. 2020. PMID: 32296146 No abstract available.
-
Invasive Versus Conservative Management of Stable Coronary Artery Disease in CKD.Am J Kidney Dis. 2021 Jan;77(1):149-151. doi: 10.1053/j.ajkd.2020.06.007. Epub 2020 Jun 30. Am J Kidney Dis. 2021. PMID: 32615149 Free PMC article. No abstract available.
-
In patients with coronary disease and CKD, initial invasive therapy did not improve angina-related health status.Ann Intern Med. 2020 Aug 18;173(4):JC17. doi: 10.7326/ACPJ202008180-017. Ann Intern Med. 2020. PMID: 32805174
References
-
- Brooks MM, Frye RL, Genuth S, et al. Hypotheses, design, and methods for the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) Trial. Am J Cardiol 2006; 97: 12A: 9G–19G. - PubMed
-
- Boden WE, O’Rourke RA, Teo KK, et al. Design and rationale of the Clinical Outcomes Utilizing Revascularization and Aggressive DruG Evaluation (COURAGE) trial: Veterans Affairs cooperative studies program no. 424. Am Heart J 2006; 151: 1173–9. - PubMed
-
- Parikh CR, Coca SG, Smith GL, Vaccarino V, Krumholz HM. Impact of chronic kidney disease on health-related quality-of-life improvement after coronary artery bypass surgery. Arch Intern Med 2006; 166: 2014–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical