

Management of Coronary Disease in Patients with Advanced Kidney Disease
- PMID: 32227756
- PMCID: PMC7274537
- DOI: 10.1056/NEJMoa1915925
Management of Coronary Disease in Patients with Advanced Kidney Disease
Abstract
Background: Clinical trials that have assessed the effect of revascularization in patients with stable coronary disease have routinely excluded those with advanced chronic kidney disease.
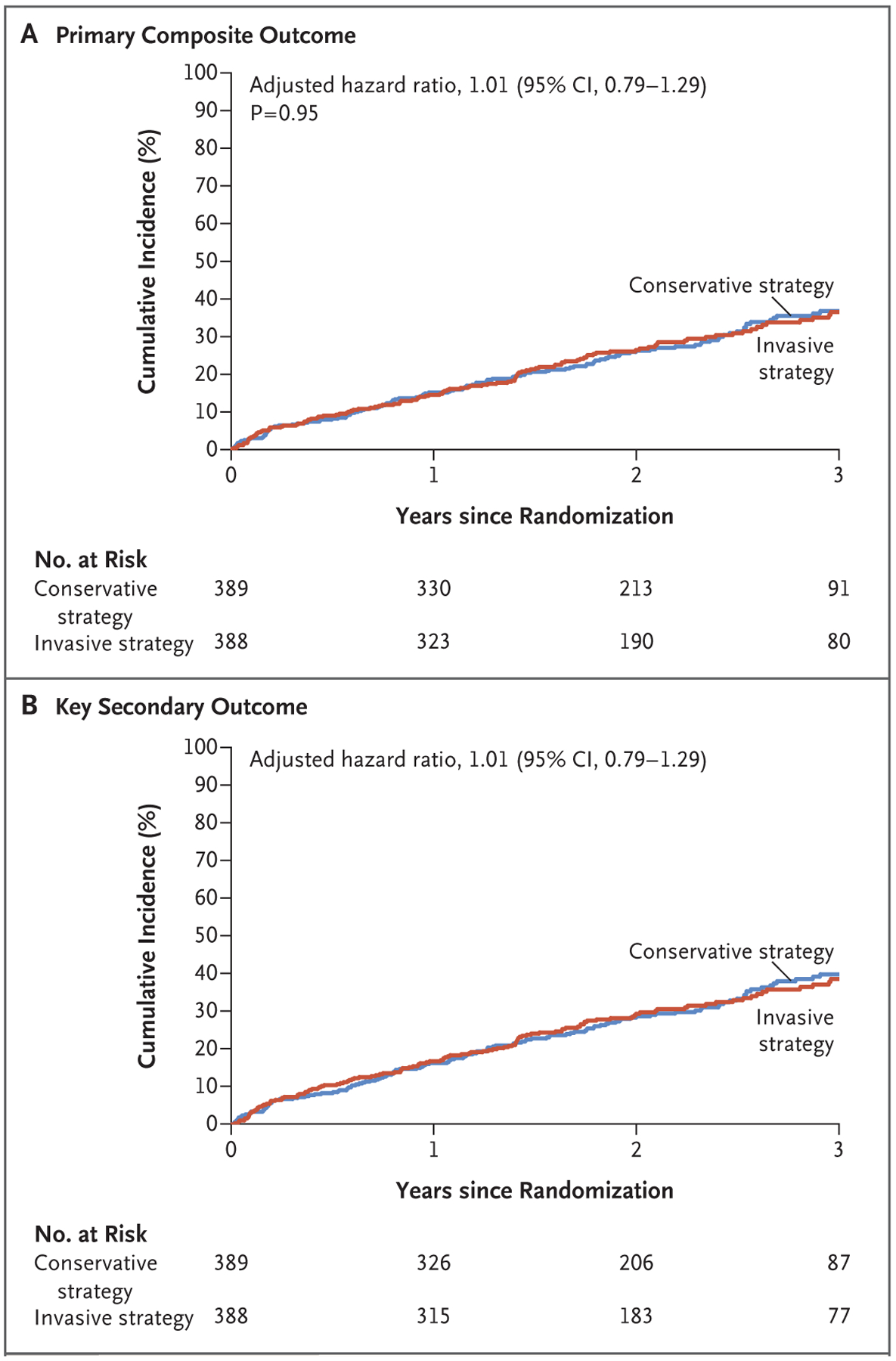
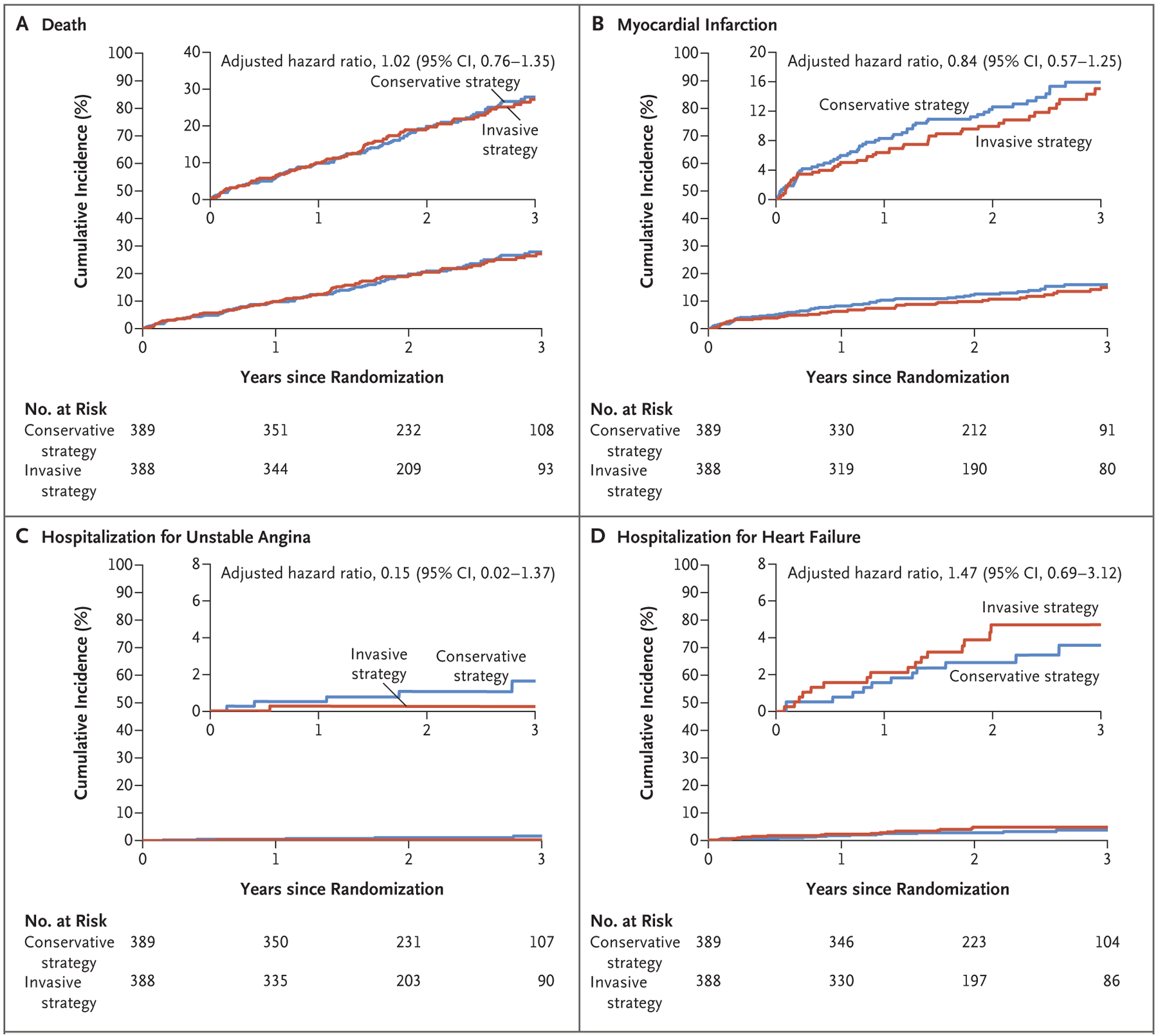
Methods: We randomly assigned 777 patients with advanced kidney disease and moderate or severe ischemia on stress testing to be treated with an initial invasive strategy consisting of coronary angiography and revascularization (if appropriate) added to medical therapy or an initial conservative strategy consisting of medical therapy alone and angiography reserved for those in whom medical therapy had failed. The primary outcome was a composite of death or nonfatal myocardial infarction. A key secondary outcome was a composite of death, nonfatal myocardial infarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest.
Results: At a median follow-up of 2.2 years, a primary outcome event had occurred in 123 patients in the invasive-strategy group and in 129 patients in the conservative-strategy group (estimated 3-year event rate, 36.4% vs. 36.7%; adjusted hazard ratio, 1.01; 95% confidence interval [CI], 0.79 to 1.29; P = 0.95). Results for the key secondary outcome were similar (38.5% vs. 39.7%; hazard ratio, 1.01; 95% CI, 0.79 to 1.29). The invasive strategy was associated with a higher incidence of stroke than the conservative strategy (hazard ratio, 3.76; 95% CI, 1.52 to 9.32; P = 0.004) and with a higher incidence of death or initiation of dialysis (hazard ratio, 1.48; 95% CI, 1.04 to 2.11; P = 0.03).
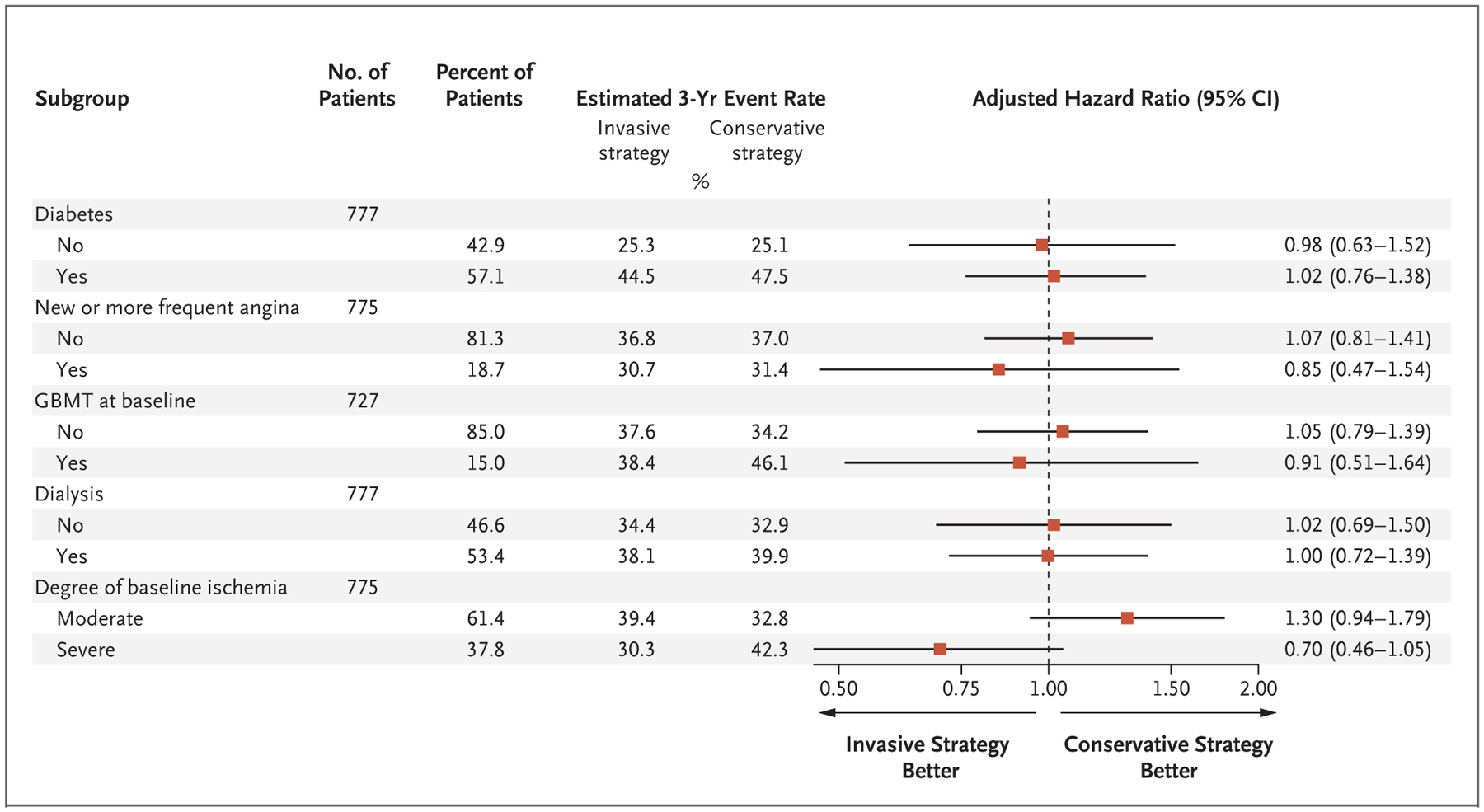
Conclusions: Among patients with stable coronary disease, advanced chronic kidney disease, and moderate or severe ischemia, we did not find evidence that an initial invasive strategy, as compared with an initial conservative strategy, reduced the risk of death or nonfatal myocardial infarction. (Funded by the National Heart, Lung, and Blood Institute and others; ISCHEMIA-CKD ClinicalTrials.gov number, NCT01985360.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
No benefit of initial invasive strategy for managing CAD in advanced CKD.Nat Rev Cardiol. 2020 Jun;17(6):320-321. doi: 10.1038/s41569-020-0384-x. Nat Rev Cardiol. 2020. PMID: 32296146 No abstract available.
-
In patients with coronary disease and CKD, adding an invasive strategy to MT did not improve outcomes.Ann Intern Med. 2020 Aug 18;173(4):JC16. doi: 10.7326/ACPJ202008180-016. Ann Intern Med. 2020. PMID: 32805175
-
Management of Coronary Disease in Patients with Advanced Kidney Disease.N Engl J Med. 2020 Sep 10;383(11):1090. doi: 10.1056/NEJMc2024023. N Engl J Med. 2020. PMID: 32905686 No abstract available.
-
Management of Coronary Disease in Patients with Advanced Kidney Disease.N Engl J Med. 2020 Sep 10;383(11):1090. doi: 10.1056/NEJMc2024023. N Engl J Med. 2020. PMID: 32905687 No abstract available.
-
Management of Coronary Disease in Patients with Advanced Kidney Disease.N Engl J Med. 2020 Sep 10;383(11):1090-1091. doi: 10.1056/NEJMc2024023. N Engl J Med. 2020. PMID: 32905688 No abstract available.
-
Management of Coronary Disease in Patients with Advanced Kidney Disease.N Engl J Med. 2020 Sep 10;383(11):1091. doi: 10.1056/NEJMc2024023. N Engl J Med. 2020. PMID: 32905689 No abstract available.
References
-
- Sarnak MJ, Amann K, Bangalore S, et al. Chronic kidney disease and coronary artery disease: JACC state-of-the-art review. J Am Coll Cardiol 2019; 74: 1823–38. - PubMed
-
- Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007; 356: 1503–16. - PubMed
-
- Zannad F, Rossignol P. Cardiovascular outcome trials in patients with advanced kidney disease: time for action. Circulation 2017; 135: 1769–71. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical