

COVID-19, ACE2, and the cardiovascular consequences
- PMID: 32228252
- PMCID: PMC7191628
- DOI: 10.1152/ajpheart.00217.2020
COVID-19, ACE2, and the cardiovascular consequences
Abstract
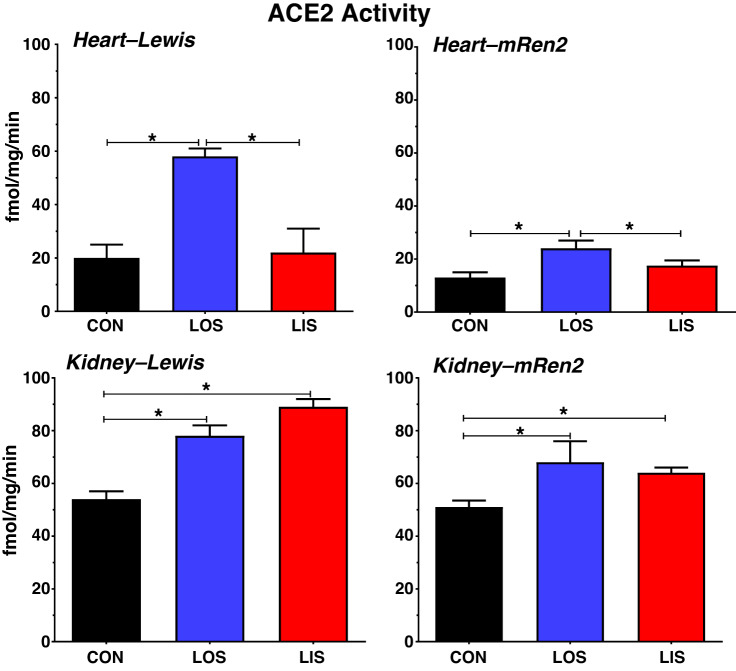
The novel SARS coronavirus SARS-CoV-2 pandemic may be particularly deleterious to patients with underlying cardiovascular disease (CVD). The mechanism for SARS-CoV-2 infection is the requisite binding of the virus to the membrane-bound form of angiotensin-converting enzyme 2 (ACE2) and internalization of the complex by the host cell. Recognition that ACE2 is the coreceptor for the coronavirus has prompted new therapeutic approaches to block the enzyme or reduce its expression to prevent the cellular entry and SARS-CoV-2 infection in tissues that express ACE2 including lung, heart, kidney, brain, and gut. ACE2, however, is a key enzymatic component of the renin-angiotensin-aldosterone system (RAAS); ACE2 degrades ANG II, a peptide with multiple actions that promote CVD, and generates Ang-(1-7), which antagonizes the effects of ANG II. Moreover, experimental evidence suggests that RAAS blockade by ACE inhibitors, ANG II type 1 receptor antagonists, and mineralocorticoid antagonists, as well as statins, enhance ACE2 which, in part, contributes to the benefit of these regimens. In lieu of the fact that many older patients with hypertension or other CVDs are routinely treated with RAAS blockers and statins, new clinical concerns have developed regarding whether these patients are at greater risk for SARS-CoV-2 infection, whether RAAS and statin therapy should be discontinued, and the potential consequences of RAAS blockade to COVID-19-related pathologies such as acute and chronic respiratory disease. The current perspective critically examines the evidence for ACE2 regulation by RAAS blockade and statins, the cardiovascular benefits of ACE2, and whether ACE2 blockade is a viable approach to attenuate COVID-19.
Keywords: ACE2; ANG II; COVID-19; SARS-CoV-2; renin-angiotensin system; statins.
Conflict of interest statement
No conflicts of interest are declared by the authors.
Figures

References
-
- Chappell MC, Marshall AC, Alzayadneh EM, Shaltout HA, Diz DI. Update on the Angiotensin converting enzyme 2-Angiotensin (1-7)-MAS receptor axis: fetal programing, sex differences, and intracellular pathways. Front Endocrinol (Lausanne) 4: 201–215, 2014. doi: 10.3389/fendo.2013.00201. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous