

Microbial burden and viral exacerbations in a longitudinal multicenter COPD cohort
- PMID: 32228581
- PMCID: PMC7104712
- DOI: 10.1186/s12931-020-01340-0
Microbial burden and viral exacerbations in a longitudinal multicenter COPD cohort
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is a heterogeneous disease characterized by frequent exacerbation phenotypes independent of disease stage. Increasing evidence shows that the microbiota plays a role in disease progression and severity, but long-term and international multicenter assessment of the variations in viral and bacterial communities as drivers of exacerbations are lacking.
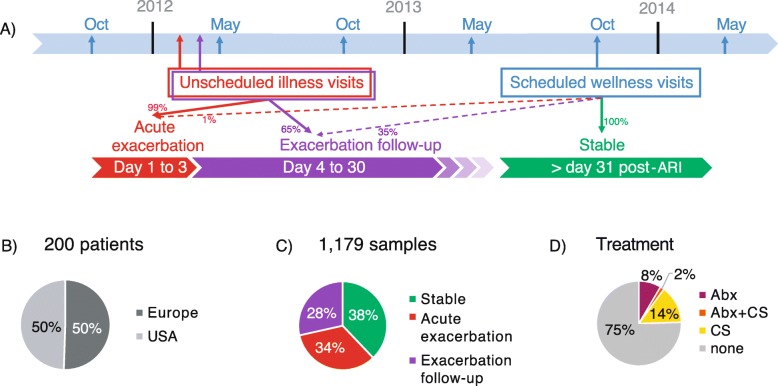
Methods: Two-hundred severe COPD patients from Europe and North America were followed longitudinally for 3 years. We performed nucleic acid detection for 20 respiratory viruses and 16S ribosomal RNA gene sequencing to evaluate the bacterial microbiota in 1179 sputum samples collected at stable, acute exacerbation and follow-up visits.
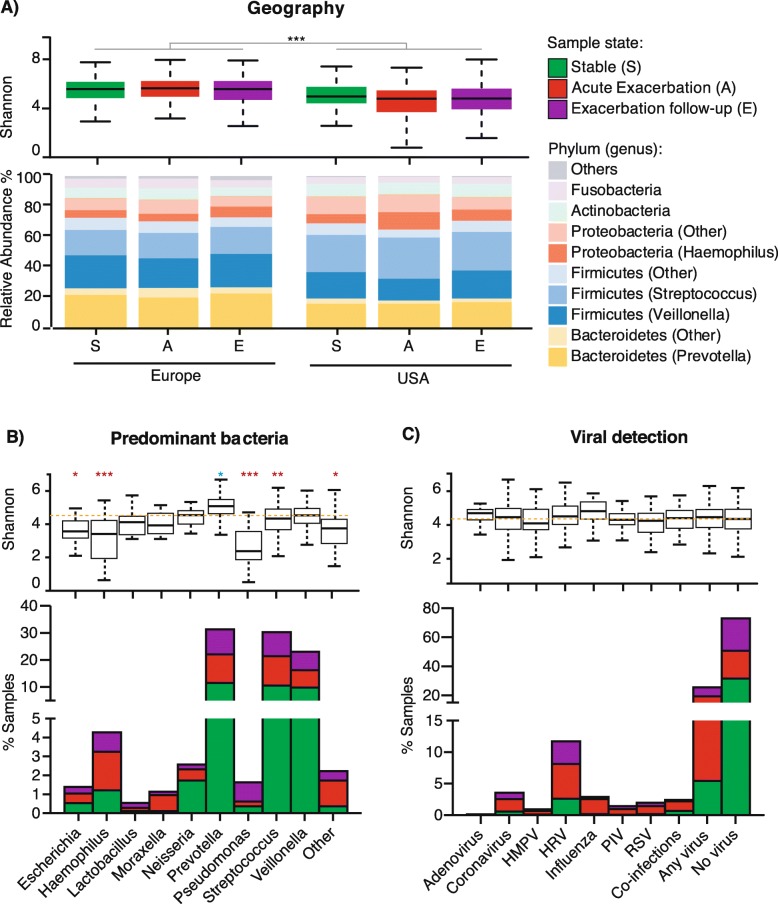
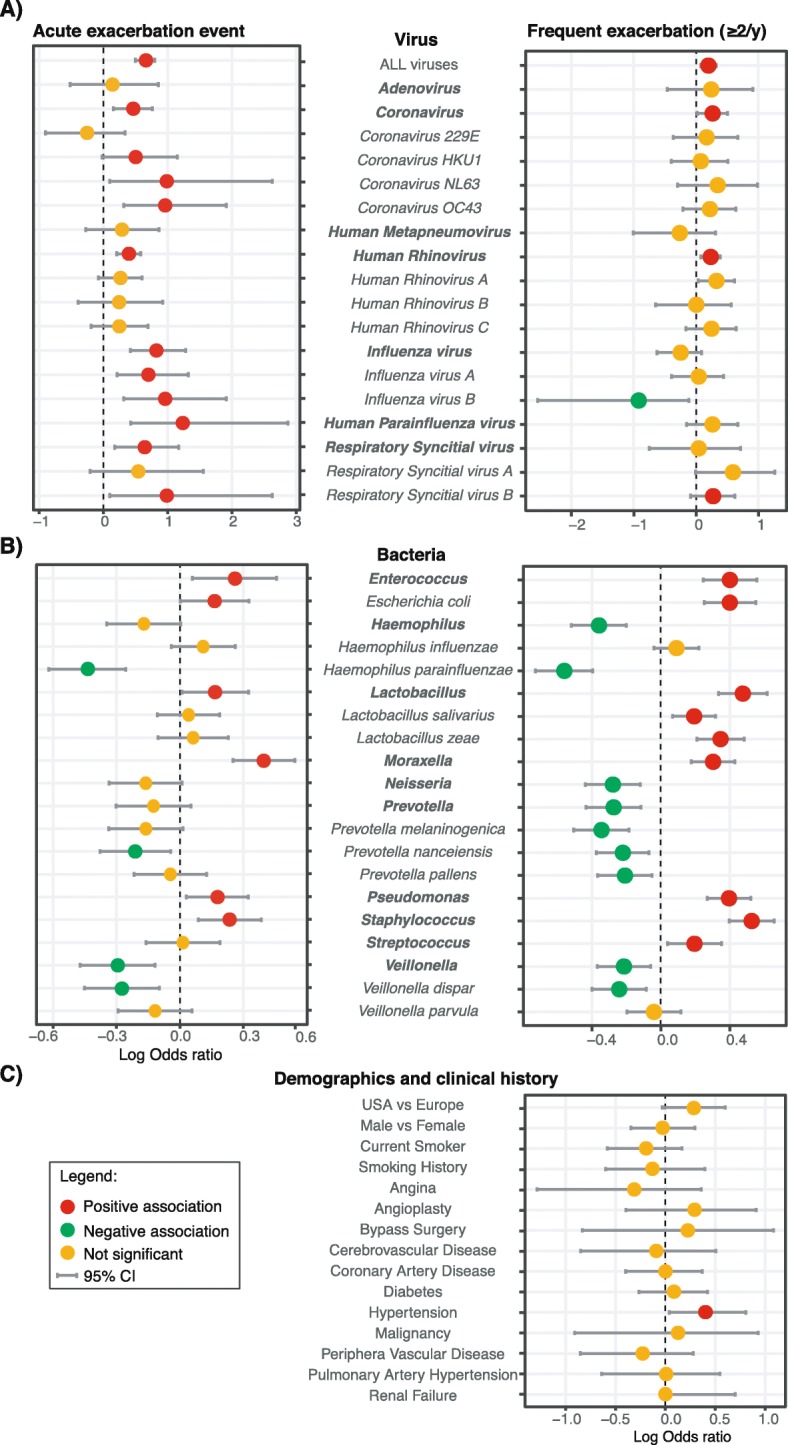
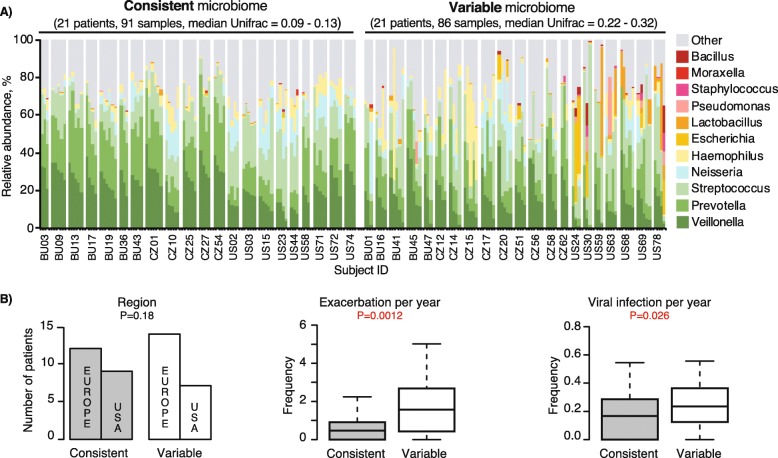
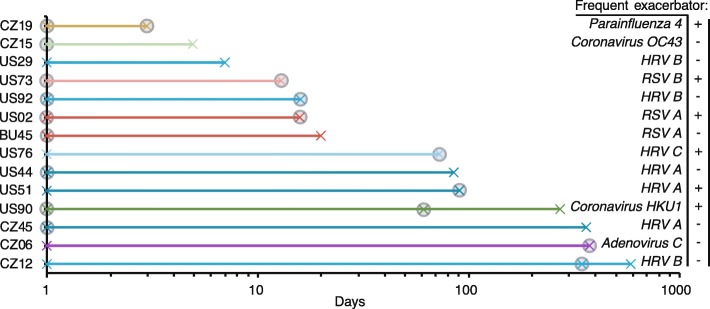
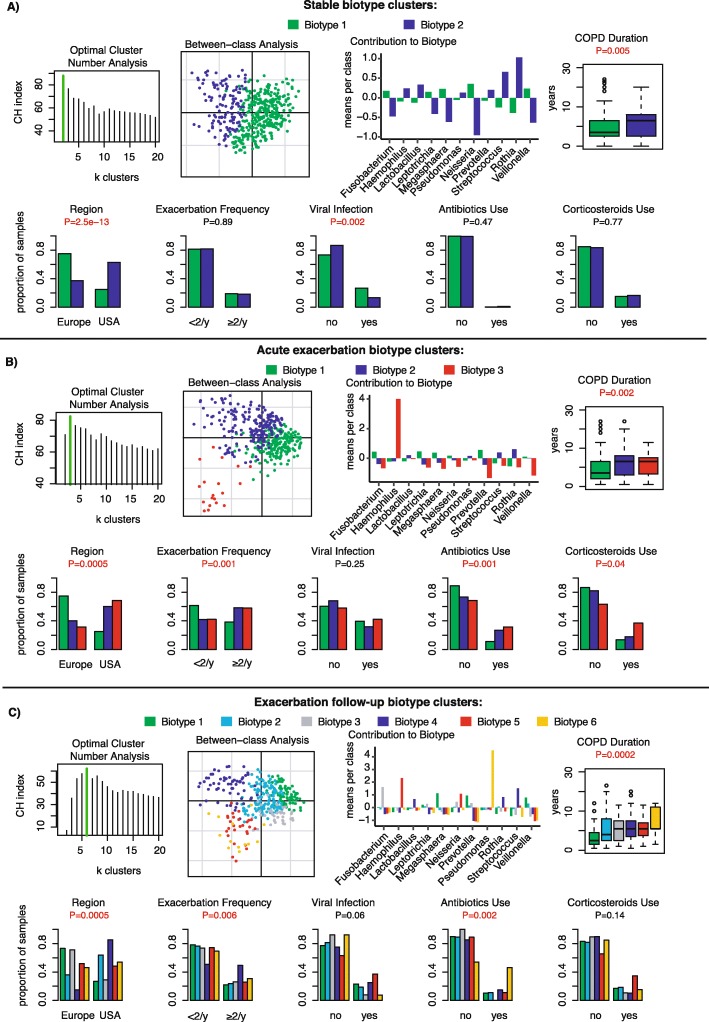
Results: Similar viral and bacterial taxa were found in patients from the USA compared to Bulgaria and Czech Republic but their microbiome diversity was significantly different (P < 0.001) and did not impact exacerbation rates. Virus infection was strongly associated with exacerbation events (P < 5E-20). Human rhinovirus (13.1%), coronavirus (5.1%) and influenza virus (3.6%) constitute the top viral pathogens in triggering exacerbation. Moraxella and Haemophilus were 5-fold and 1.6-fold more likely to be the dominating microbiota during an exacerbation event. Presence of Proteobacteria such as Pseudomonas or Staphylococcus amongst others, were associated with exacerbation events (OR > 0.17; P < 0.02) but more strongly associated with exacerbation frequency (OR > 0.39; P < 4E-10), as confirmed by longitudinal variations and biotyping of the bacterial microbiota, and suggesting a role of the microbiota in sensitizing the lung.
Conclusions: This study highlights bacterial taxa in lung sensitization and viral triggers in COPD exacerbations. It provides a global overview of the diverse targets for drug development and explores new microbiome analysis methods to guide future patient management applications.
Conflict of interest statement
All authors are employees and share holders of AstraZeneca.
Figures
References
-
- Agusti A, Calverley PMA, Celli B, Coxson HO, Edwards LD, Lomas DA, MacNee W, Miller BE, Rennard S, Silverman EK, Tal-Singer R, Wouters E, Yates JC, Vestbo J. Evaluation of COPD longitudinally to identify predictive surrogate endpoints (ECLIPSE) investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11:122. doi: 10.1186/1465-9921-11-122. - DOI - PMC - PubMed
-
- Hurst JR, Vestbo J, Anzueto A, Locantore NW, Müllerova H, Tal-Singer R, Miller BE, Lomas DA, Agusti A, MacNee W, Calverley PMA, Rennard SI, Wouters EFM, Wedzicha JA. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. doi: 10.1056/NEJMoa0909883. - DOI - PubMed
-
- Ghebre MA, Pang PH, Diver S, Desai D, Bafadhel M, Haldar K, Kebadze T, Cohen S, Newbold P, Rapley L, Woods J, Rugman P, Pavord ID, Johnston SL, Barer M, May RD, Brightling CE. Biological exacerbation clusters demonstrate asthma and chronic obstructive pulmonary disease overlap with distinct mediator and microbiome profiles. J Allergy Clin Immunol. 2018;141:2027–2036.e12. doi: 10.1016/j.jaci.2018.04.013. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
