

Pre-hospital CPR and early REBOA in trauma patients - results from the ABOTrauma Registry
- PMID: 32228640
- PMCID: PMC7104487
- DOI: 10.1186/s13017-020-00301-8
Pre-hospital CPR and early REBOA in trauma patients - results from the ABOTrauma Registry
Abstract
Background: Severely injured trauma patients suffering from traumatic cardiac arrest (TCA) and requiring cardiopulmonary resuscitation (CPR) rarely survive. The role of resuscitative endovascular balloon occlusion of the aorta (REBOA) performed early after hospital admission in patients with TCA is not well-defined. As the use of REBOA increases, there is great interest in knowing if there is a survival benefit related to the early use of REBOA after TCA. Using data from the ABOTrauma Registry, we aimed to study the role of REBOA used early after hospital admission in trauma patients who required pre-hospital CPR.
Methods: Retrospective and prospective data on the use of REBOA were collected from the ABOTrauma Registry from 11 centers in seven countries globally between 2014 and 2019. In all patients with pre-hospital TCA, the predicted probability of survival, calculated with the Revised Injury Severity Classification II (RISC II), was compared with the observed survival rate.
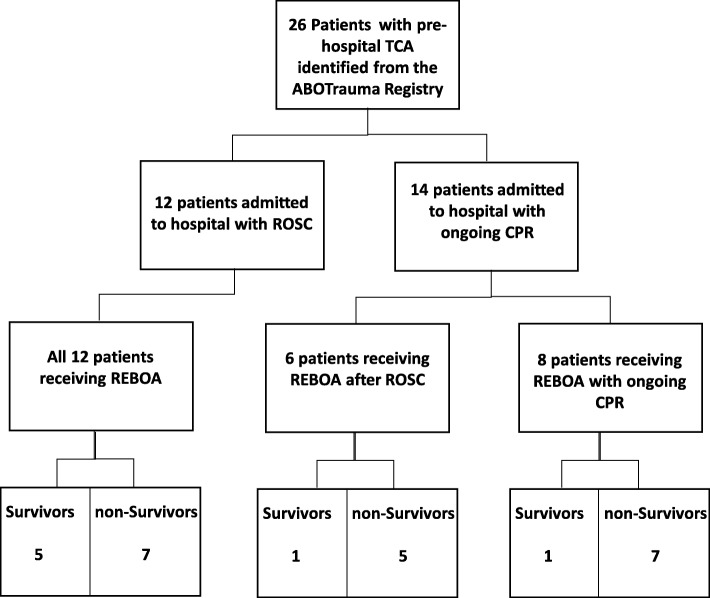
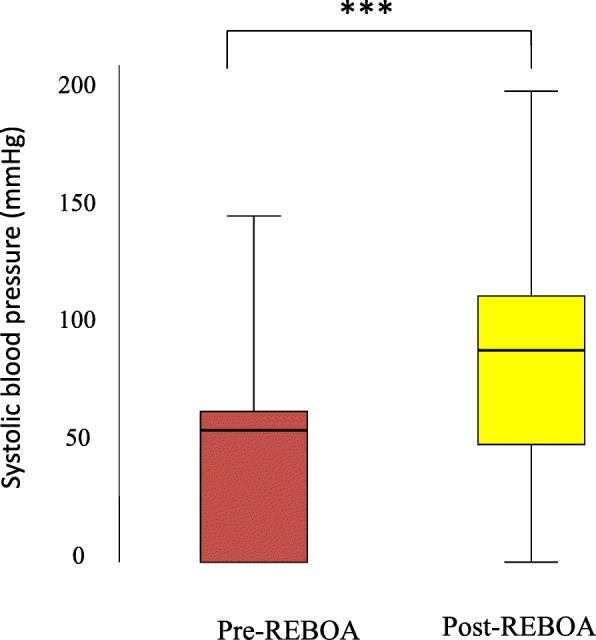
Results: Of 213 patients in the ABOTrauma Registry, 26 patients (12.2%) who had received pre-hospital CPR were identified. The median (range) Injury Severity Score (ISS) was 45.5 (25-75). Fourteen patients (54%) had been admitted to the hospital with ongoing CPR. Nine patients (35%) died within the first 24 h, while seventeen patients (65%) survived post 24 h. The survival rate to hospital discharge was 27% (n = 7). The predicted mortality using the RISC II was 0.977 (25 out of 26). The observed mortality (19 out of 26) was significantly lower than the predicted mortality (p = 0.049). Patients not responding to REBOA were more likely to die. Only one (10%) out of 10 non-responders survived. The survival rate in the 16 patients responding to REBOA was 37.5% (n = 6). REBOA with a median (range) duration of 45 (8-70) minutes significantly increases blood pressure from the median (range) 56.5 (0-147) to 90 (0-200) mmHg.
Conclusions: Mortality in patients suffering from TCA and receiving REBOA early after hospital admission is significantly lower than predicted by the RISC II. REBOA may improve survival after TCA. The use of REBOA in these patients should be further investigated.
Keywords: CPR; Cardiac arrest; Endovascular resuscitation; REBOA; Trauma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Harris T, Masud S, Lamond A, Abu-Habsa M. Traumatic cardiac arrest: a unique approach. Eur J Emerg Med. 2015;22(2):72–78. - PubMed
-
- McGreevy DT, Abu-Zidan FM, Sadeghi M, Pirouzram A, Toivola A, Skoog P, et al. Feasibility and clinical outcome of REBOA in patients with impending traumatic cardiac arrest. Shock. 2019. - PubMed
-
- Truhlar A, Deakin CD, Soar J, Khalifa GE, Alfonzo A, Bierens JJ, et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. Resuscitation. 2015;95:148–201. - PubMed
-
- Burlew CC, Moore EE, Moore FA, Coimbra R, McIntyre RC, Jr, Davis JW, et al. Western Trauma Association critical decisions in trauma: resuscitative thoracotomy. J Trauma Acute Care Surg. 2012;73(6):1359–1363. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
