

Durable Survival Outcomes in Primary and Secondary Central Nervous System Lymphoma After High-dose Chemotherapy and Autologous Stem Cell Transplantation Using a Thiotepa, Busulfan, and Cyclophosphamide Conditioning Regimen
- PMID: 32229199
- PMCID: PMC7138188
- DOI: 10.1016/j.clml.2020.02.009
Durable Survival Outcomes in Primary and Secondary Central Nervous System Lymphoma After High-dose Chemotherapy and Autologous Stem Cell Transplantation Using a Thiotepa, Busulfan, and Cyclophosphamide Conditioning Regimen
Abstract
Background: High-dose chemotherapy (HDC) with autologous stem cell transplantation (ASCT) has been investigated in patients with primary central nervous system lymphoma (PCNSL) and non-Hodgkin lymphoma (NHL) with CNS involvement and has shown promising results.
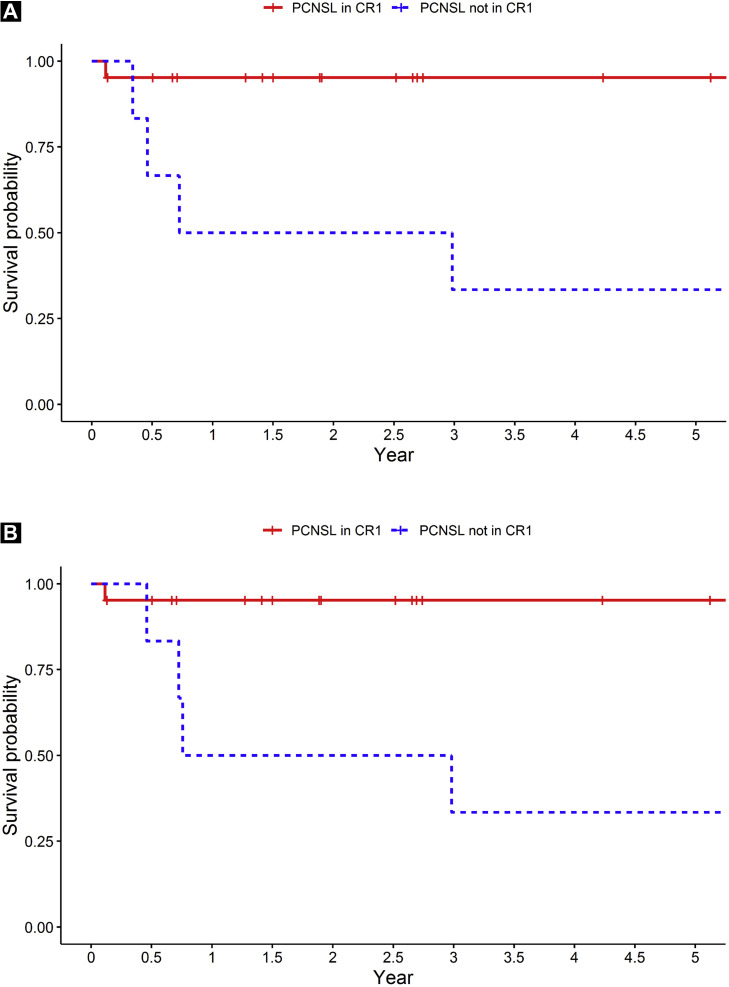
Patients and methods: A retrospective analysis was performed of 48 consecutive patients who had undergone HDC/ASCT with TBC (thiotepa, busulfan, cyclophosphamide) conditioning for PCNSL (27 patients), secondary CNS lymphoma (SCNSL) (8 patients), or relapsed disease with CNS involvement (13 patients) from July 2006 to December 2017. Of the 27 patients with PCNSL, 21 had undergone ASCT at first complete remission (CR1).
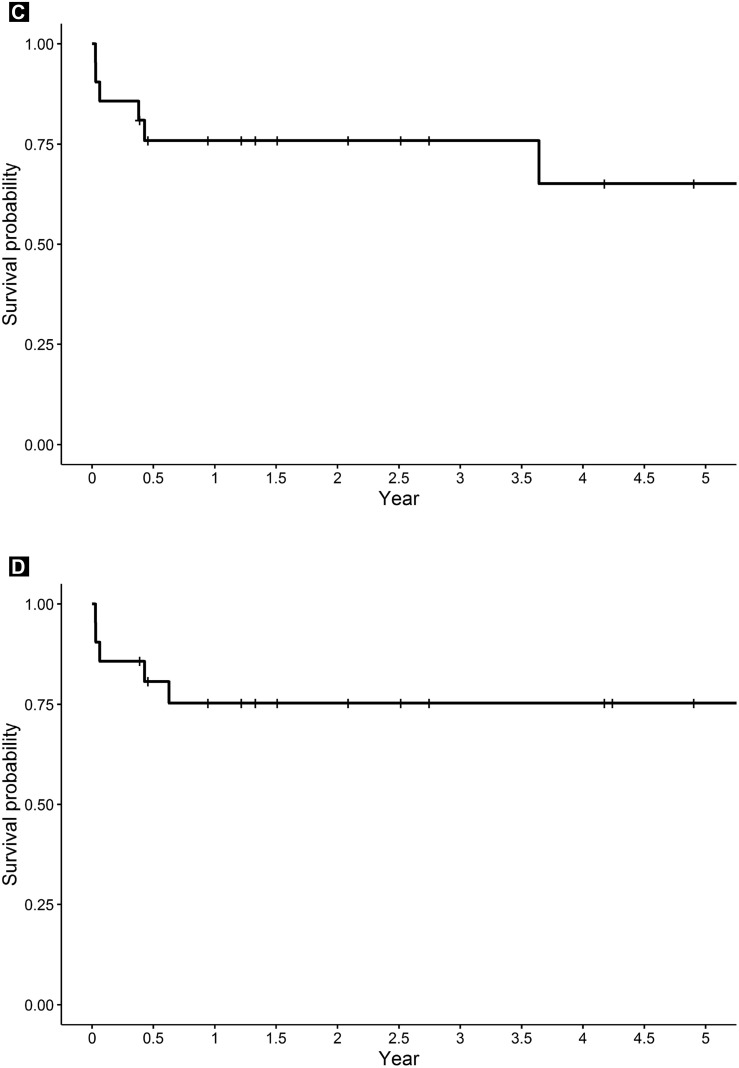
Results: The 2-year progression-free survival (PFS) rate was 80.5% (95% confidence interval [CI], 69.9-92.9) and the 2-year overall survival (OS) rate was 80.1% (95% CI, 69.2%-92.7%) among all patients. The 2-year PFS and OS rate for patients with PCNSL in CR1 was 95.2% (95% CI, 86.6%-100%) and 95.2% (95% CI, 86.6%-100%), respectively. On univariate analysis of the patients with PCNSL, ASCT in CR1 was the only variable statistically significant for outcome (P = .007 for PFS; P = .008 for OS). Among patients with SCNSL or CNS relapse, the 2-year PFS and OS rate were comparable at 75.9% (95% CI, 59.5%-96.8%) and 75.3% (95% CI, 58.6%-98.6%), respectively. The most common side effects were febrile neutropenia (89.6%; of which 66.7% had an infectious etiology identified), nausea/vomiting (85.4%), diarrhea (93.8%), mucositis (89.6%), and electrolyte abnormalities (89.6%). Four patients (8.3%) died of treatment-related overwhelming infection; of these patients, 3 had SCNSL.
Conclusion: HDC and ASCT using TBC conditioning for both PCNSL and secondary CNS NHL appears to have encouraging long-term efficacy with manageable side effects.
Keywords: ASCT; Non-Hodgkin lymphoma; PCNSL; Relapse; SCNL.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Citterio G., Reni M., Gatta G., Ferreri A.J.M. Primary central nervous system lymphoma. Crit Rev Oncol Hematol. 2017;113:97–110. - PubMed
-
- Thiel E., Korfel A., Martus P. High-dose methotrexate with or without whole brain radiotherapy for primary CNS lymphoma (G-PCNSL-SG-1): a phase 3, randomised, non-inferiority trial. Lancet Oncol. 2010;11:1036–1047. - PubMed
-
- Korfel A., Thiel E., Martus P. Randomized phase III study of whole-brain radiotherapy for primary CNS lymphoma. Neurology. 2015;84:1242–1248. - PubMed
-
- Abrey L.E., Moskowitz C.H., Mason W.P. Intensive methotrexate and cytarabine followed by high-dose chemotherapy with autologous stem-cell rescue in patients with newly diagnosed primary CNS lymphoma: an intent-to-treat analysis. J Clin Oncol. 2003;21:4151–4156. - PubMed
