

Protocol for a randomised trial of an interprofessional team-delivered intervention to support surrogate decision-makers in ICUs
- PMID: 32229520
- PMCID: PMC7170558
- DOI: 10.1136/bmjopen-2019-033521
Protocol for a randomised trial of an interprofessional team-delivered intervention to support surrogate decision-makers in ICUs
Abstract
Introduction: Although shortcomings in clinician-family communication and decision making for incapacitated, critically ill patients are common, there are few rigorously tested interventions to improve outcomes. In this manuscript, we present our methodology for the Pairing Re-engineered Intensive Care Unit Teams with Nurse-Driven Emotional support and Relationship Building (PARTNER 2) trial, and discuss design challenges and their resolution.
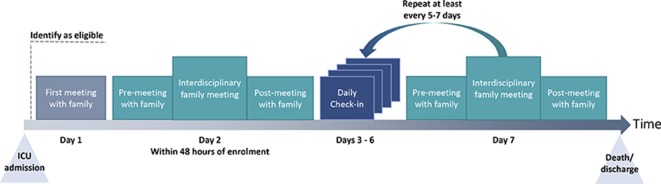
Methods and analysis: This is a pragmatic, stepped-wedge, cluster randomised controlled trial comparing the PARTNER 2 intervention to usual care among 690 incapacitated, critically ill patients and their surrogates in five ICUs in Pennsylvania. Eligible subjects will include critically ill patients at high risk of death and/or severe long-term functional impairment, their main surrogate decision-maker and their clinicians. The PARTNER intervention is delivered by the interprofessional ICU team and overseen by 4-6 nurses from each ICU. It involves: (1) advanced communication skills training for nurses to deliver support to surrogates throughout the ICU stay; (2) deploying a structured family support pathway; (3) enacting strategies to foster collaboration between ICU and palliative care services and (4) providing intensive implementation support to each ICU to incorporate the family support pathway into clinicians' workflow. The primary outcome is surrogates' ratings of the quality of communication during the ICU stay as assessed by telephone at 6-month follow-up. Prespecified secondary outcomes include surrogates' scores on the Hospital Anxiety and Depression Scale, the Impact of Event Scale, the modified Patient Perception of Patient Centredness scale, the Decision Regret Scale, nurses' scores on the Maslach Burnout Inventory, and length of stay during and costs of the index hospitalisation.We also discuss key methodological challenges, including determining the optimal level of randomisation, using existing staff to deploy the intervention and maximising long-term follow-up of participants.
Ethics and dissemination: We obtained ethics approval through the University of Pittsburgh, Human Research Protection Office. The findings will be published in peer-reviewed journals.
Trial registration number: NCT02445937.
Keywords: adult intensive & critical care; adult palliative care; clinical trials; communication; nursing; statistics and research methods.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Bedell SE, Pelle D, Maher PL, et al. Do-Not-Resuscitate orders for critically ill patients in the hospital. how are they used and what is their impact? JAMA 1986;256:233–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical