

Cancer Cachexia and Related Metabolic Dysfunction
- PMID: 32230855
- PMCID: PMC7177950
- DOI: 10.3390/ijms21072321
Cancer Cachexia and Related Metabolic Dysfunction
Abstract
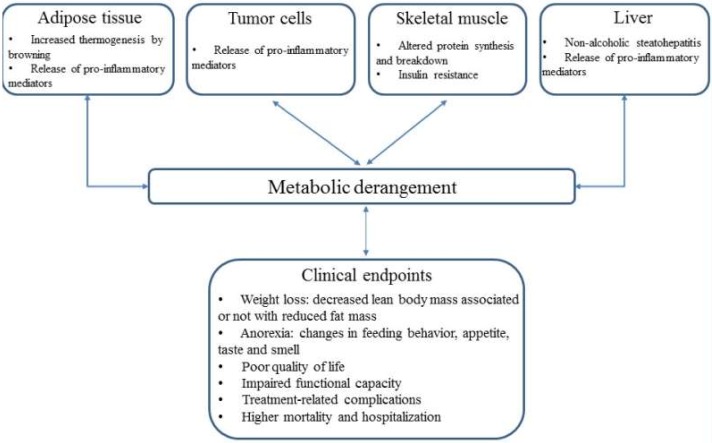
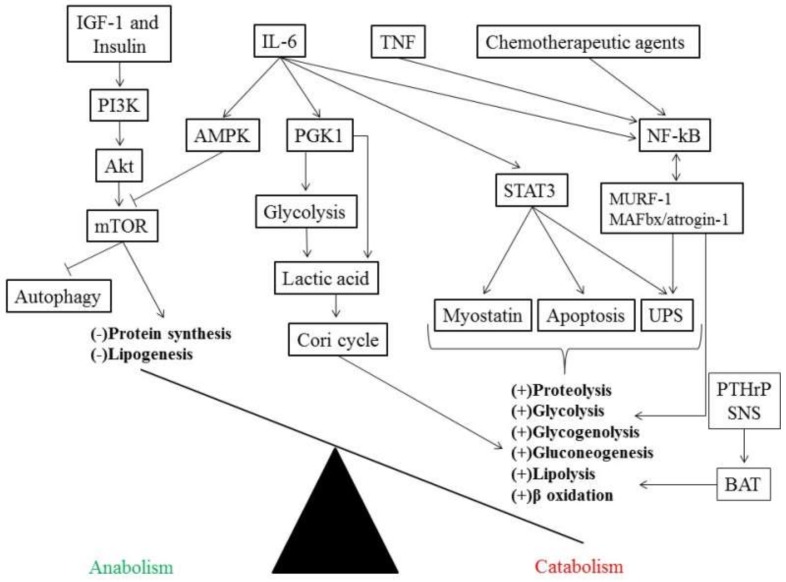
Cancer cachexia is a complex multifactorial syndrome marked by a continuous depletion of skeletal muscle mass associated, in some cases, with a reduction in fat mass. It is irreversible by nutritional support alone and affects up to 74% of patients with cancer-dependent on the underlying type of cancer-and is associated with physical function impairment, reduced response to cancer-related therapy, and higher mortality. Organs, like muscle, adipose tissue, and liver, play an important role in the progression of cancer cachexia by exacerbating the pro- and anti-inflammatory response initially activated by the tumor and the immune system of the host. Moreover, this metabolic dysfunction is produced by alterations in glucose, lipids, and protein metabolism that, when maintained chronically, may lead to the loss of skeletal muscle and adipose tissue. Although a couple of drugs have yielded positive results in increasing lean body mass with limited impact on physical function, a single therapy has not lead to effective treatment of this condition. Therefore, a multimodal intervention, including pharmacological agents, nutritional support, and physical exercise, may be a reasonable approach for future studies to better understand and prevent the wasting of body compartments in patients with cancer cachexia.
Keywords: cancer cachexia; clinical management; inflammation; metabolic dysfunction; metabolism.
Conflict of interest statement
S.v.H has been a paid consultant for and/or received honoraria payments from Bayer, Boehringer Ingelheim, BRAHMS, Chugai, Grünenthal, Helsinn, Hexal, Novartis, Respicardia, Roche, Sorin, and Vifor. S.v.H owns shares in Actimed. S.v.H reports research support from IMI and the German Center for Cardiovascular Research (DZHK). M.L. has been a paid consultant for and/or received honoraria payments from Astra Zeneca, Boehringer Ingelheim, Novartis, Roche, and Vifor. M.L. owns shares in Actimed. M.L. reports research support from Slovenian Research Agency. J.F. reports research support from Slovenian Research Agency.
Figures
References
-
- Anker M.S., Holcomb R., Muscaritoli M., von Haehling S., Haverkamp W., Jatoi A., Morley J.E., Strasser F., Landmesser U., Coats A.J.S., et al. Orphan disease status of cancer cachexia in the USA and in the European Union: A systematic review. J. Cachexia Sarcopenia Muscle. 2019;10:22–34. doi: 10.1002/jcsm.12402. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
