

Adverse cardiac effects of cancer therapies: cardiotoxicity and arrhythmia
- PMID: 32231332
- PMCID: PMC8782611
- DOI: 10.1038/s41569-020-0348-1
Adverse cardiac effects of cancer therapies: cardiotoxicity and arrhythmia
Abstract
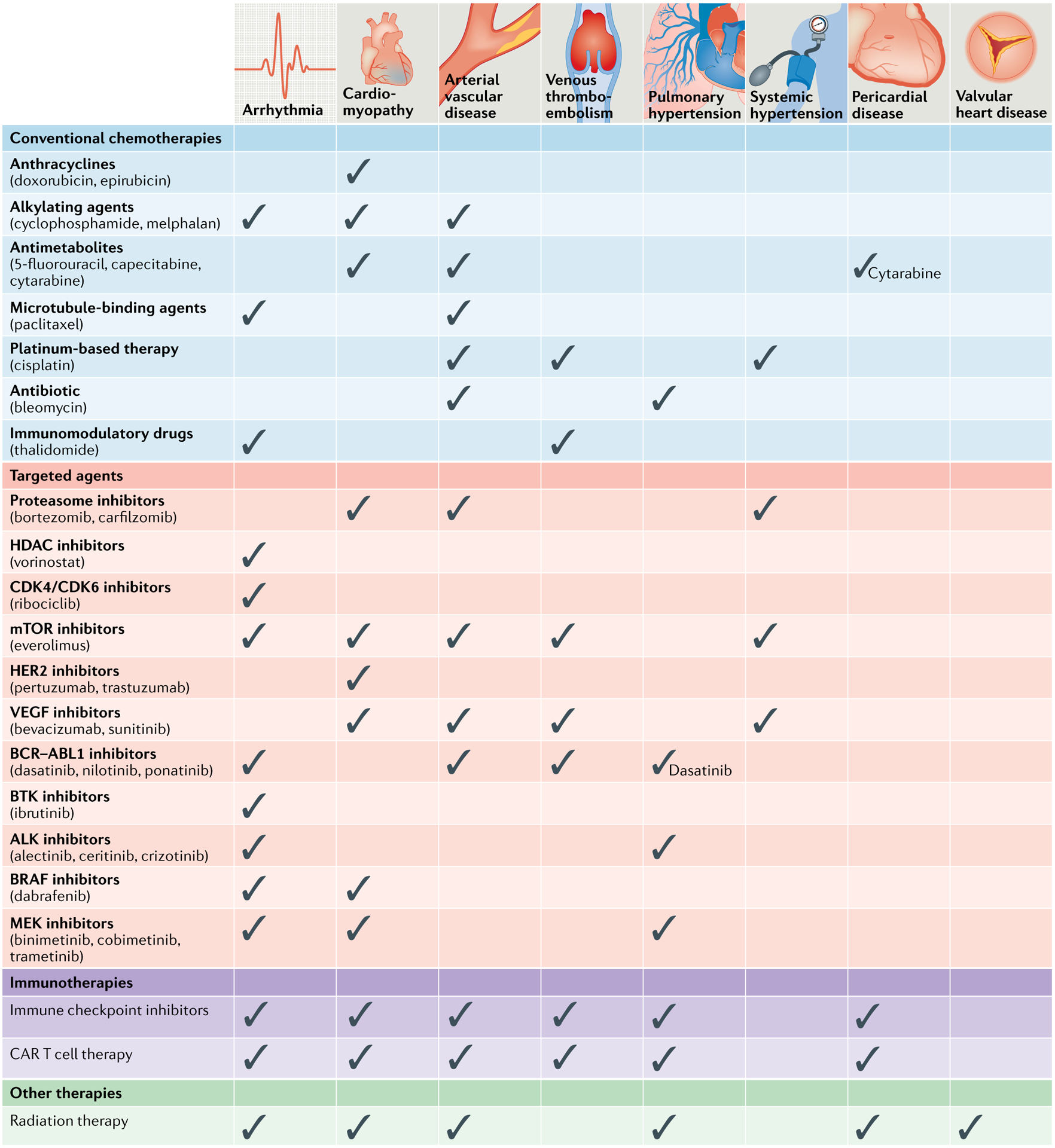
Remarkable progress has been made in the development of new therapies for cancer, dramatically changing the landscape of treatment approaches for several malignancies and continuing to increase patient survival. Accordingly, adverse effects of cancer therapies that interfere with the continuation of best-possible care, induce life-threatening risks or lead to long-term morbidity are gaining increasing importance. Cardiovascular toxic effects of cancer therapeutics and radiation therapy are the epitome of such concerns, and proper knowledge, interpretation and management are needed and have to be placed within the context of the overall care of individual patients with cancer. Furthermore, the cardiotoxicity spectrum has broadened to include myocarditis with immune checkpoint inhibitors and cardiac dysfunction in the setting of cytokine release syndrome with chimeric antigen receptor T cell therapy. An increase in the incidence of arrhythmias related to inflammation such as atrial fibrillation can also be expected, in addition to the broadening set of cancer therapeutics that can induce prolongation of the corrected QT interval. Therefore, cardiologists of today have to be familiar not only with the cardiotoxicity associated with traditional cancer therapies, such as anthracycline, trastuzumab or radiation therapy, but even more so with an ever-increasing repertoire of therapeutics. This Review provides this information, summarizing the latest developments at the juncture of cardiology, oncology and haematology.
Conflict of interest statement
Competing interests
The author declares no competing interests.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
