

Timing of Circulatory and Neurological Events in Syncope
- PMID: 32232058
- PMCID: PMC7082775
- DOI: 10.3389/fcvm.2020.00036
Timing of Circulatory and Neurological Events in Syncope
Abstract
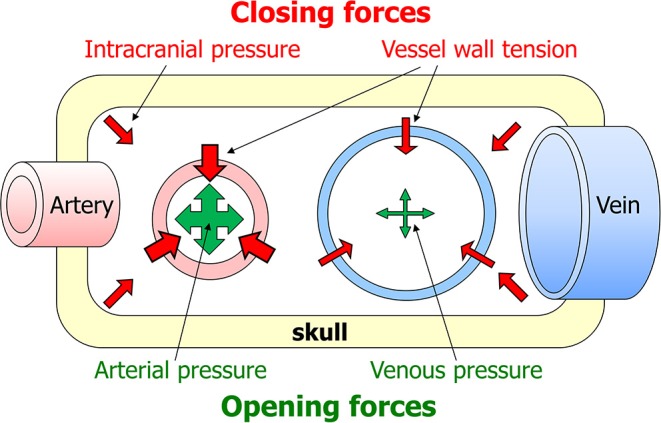
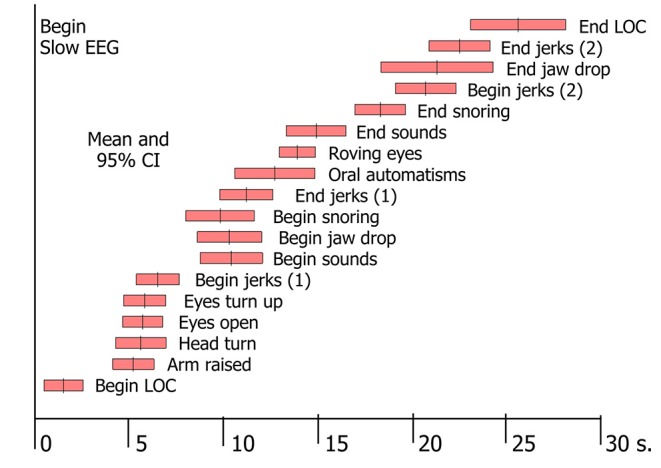
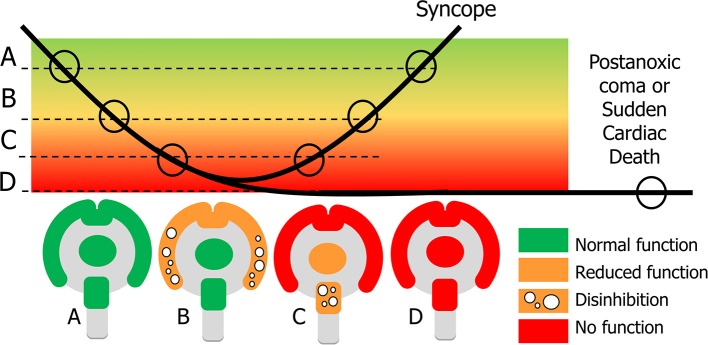
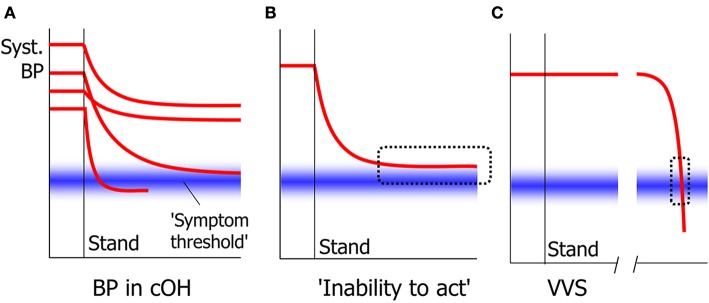
Syncope usually lasts less than a minute, in which short time arterial blood pressure temporarily falls enough to decrease brain perfusion so much that loss of consciousness ensues. Blood pressure decreases quickest when the heart suddenly stops pumping, which happens in arrhythmia and in severe cardioinhibitory reflex syncope. Loss of consciousness starts about 8 s after the last heart beat and circulatory standstill occurs after 10-15 s. A much slower blood pressure decrease can occur in syncope due to orthostatic hypotension Standing blood pressure can then stabilize at low values often causing more subtle signs (i.e., inability to act) but often not low enough to cause loss of consciousness. Cerebral autoregulation attempts to keep cerebral blood flow constant when blood pressure decreases. In reflex syncope both the quick blood pressure decrease and its low absolute value mean that cerebral autoregulation cannot prevent syncope. It has more protective value in orthostatic hypotension. Neurological signs are related to the severity and timing of cerebral hypoperfusion. Several unanswered pathophysiological questions with possible clinical implications are identified.
Keywords: pathophysiology; syncope; tilt table test; transient loss of consciousness; vasovagal syncope.
Copyright © 2020 van Dijk, van Rossum and Thijs.
Figures
References
-
- Shen WK, Sheldon RS, Benditt DG, Cohen MI, Forman DE, Goldberger ZD, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm. (2017) 14:e155–217. 10.1016/j.hrthm.2017.03.004 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources