

The Treatment of Gallstone Disease
- PMID: 32234195
- PMCID: PMC7132079
- DOI: 10.3238/arztebl.2020.0148
The Treatment of Gallstone Disease
Abstract
Background: Gallstone disease affects up to 20% of the European population, and cholelithiasis is the most common reason for hospitalization in gastroenterology.
Methods: This review is based on pertinent publications retrieved by a selective search of the literature, including the German clinical practice guidelines on the diagnosis and treatment of gallstones and corresponding guidelines from abroad.
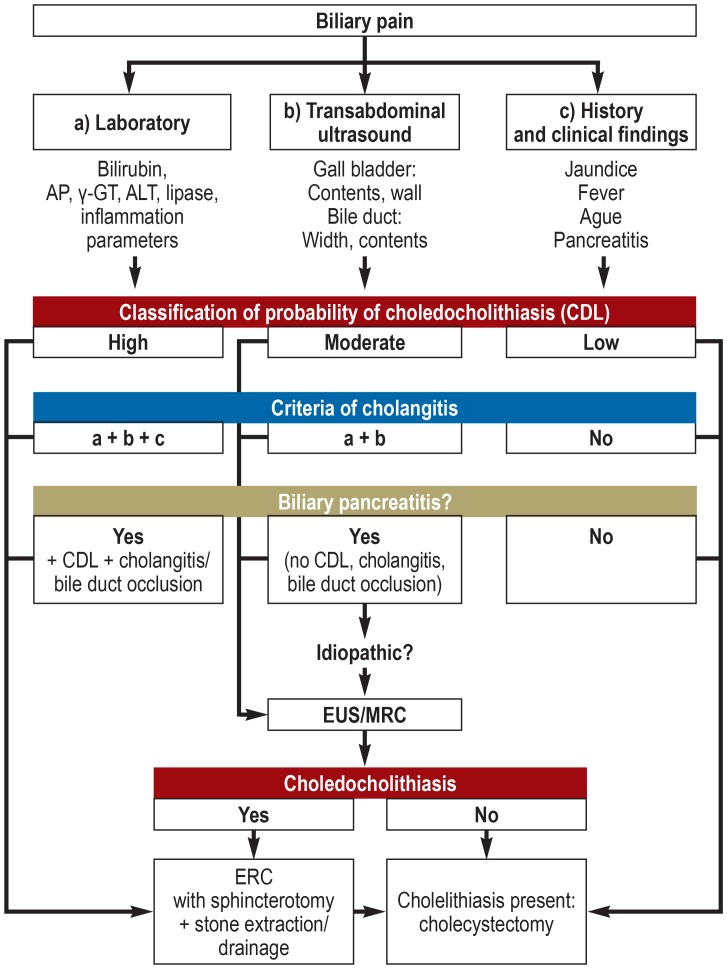
Results: Regular physical activity and an appropriate diet are the most important measures for the prevention of gallstone disease. Transcutaneous ultrasonography is the paramount method of diagnosing gallstones. Endoscopic retrograde cholangiography should only be carried out as part of a planned therapeutic intervention; endosonography beforehand lessens the number of endoscopic retrograde cholangiographies that need to be performed. Cholecystectomy is indicated for patients with symptomatic gallstones or sludge. This should be performed laparoscopically with a four-trocar technique, if possible. Routine perioperative antibiotic prophylaxis is not necessary. Cholecystectomy can be performed in any trimester of pregnancy, if urgently indicated. Acute cholecystitis is an indication for early laparoscopic cholecystectomy within 24 hours of admission to hospital. After successful endoscopic clearance of the biliary pathway, patients who also have cholelithiasis should undergo laparoscopic cholecystectomy within 72 hours.
Conclusion: The timing of treatment for gallstone disease is an essential determinant of therapeutic success.
Figures

Comment in
-
Evidence Is Needed in Support of the Indication.Dtsch Arztebl Int. 2020 Jul 6;117(27-28):490. doi: 10.3238/arztebl.2020.0490a. Dtsch Arztebl Int. 2020. PMID: 33081912 Free PMC article. No abstract available.
References
-
- European Association for the Study of the Liver (EASL) EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. J Hepatol. 2016;65:146–181. - PubMed
-
- Gutt C, Jenssen C, Barreiros AP, et al. Aktualisierte S3-Leitlinie der Deutschen Gesellschaft für Gastroenterologie, Verdauungs- und Stoffwechselkrankheiten (DGVS) und der Deutschen Gesellschaft für Allgemein- und Viszeralchirurgie (DGAV) zur Prävention, Diagnostik und Behandlung von Gallensteinen. Z Gastroenterol. 2018;56:912–966. - PubMed
-
- NICE. Clinical Guideline 188; Gallstone disease: diagnosis and management. National Institute for Health and Care Excellence. 2014
-
- Gutt CN. Akute Cholezystitis: primär konservatives oder operatives Vorgehen? Chirurg. 2013;84:185–190. - PubMed
-
- Overby DW, Apelgren KN, Richardson W, Fanelli R. Society of American Gastrointestinal and Endoscopic Surgeons: SAGES guidelines for the clinical application of laparoscopic biliary tract surgery. Surg Endosc. 2010;24:2368–2386. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources