

Physical activity and exercise: Strategies to manage frailty
- PMID: 32234291
- PMCID: PMC7284931
- DOI: 10.1016/j.redox.2020.101513
Physical activity and exercise: Strategies to manage frailty
Abstract
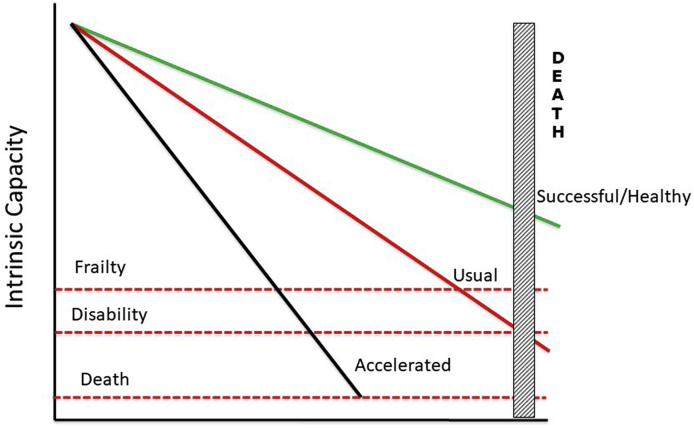
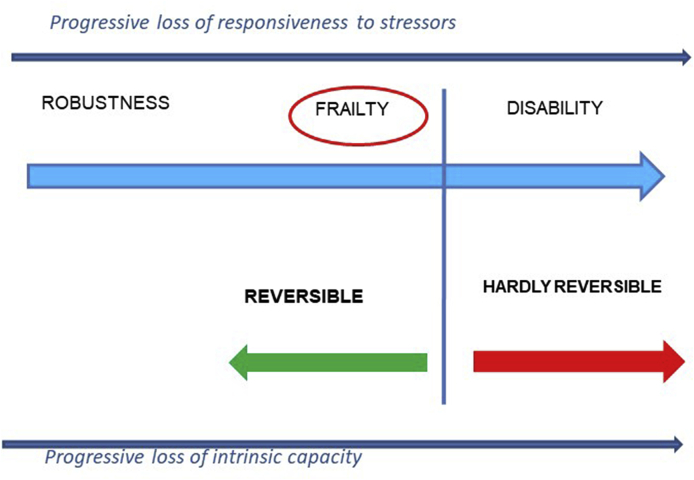
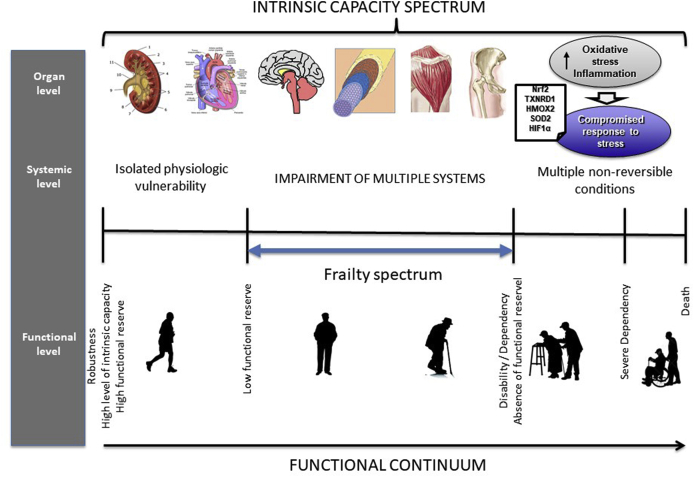
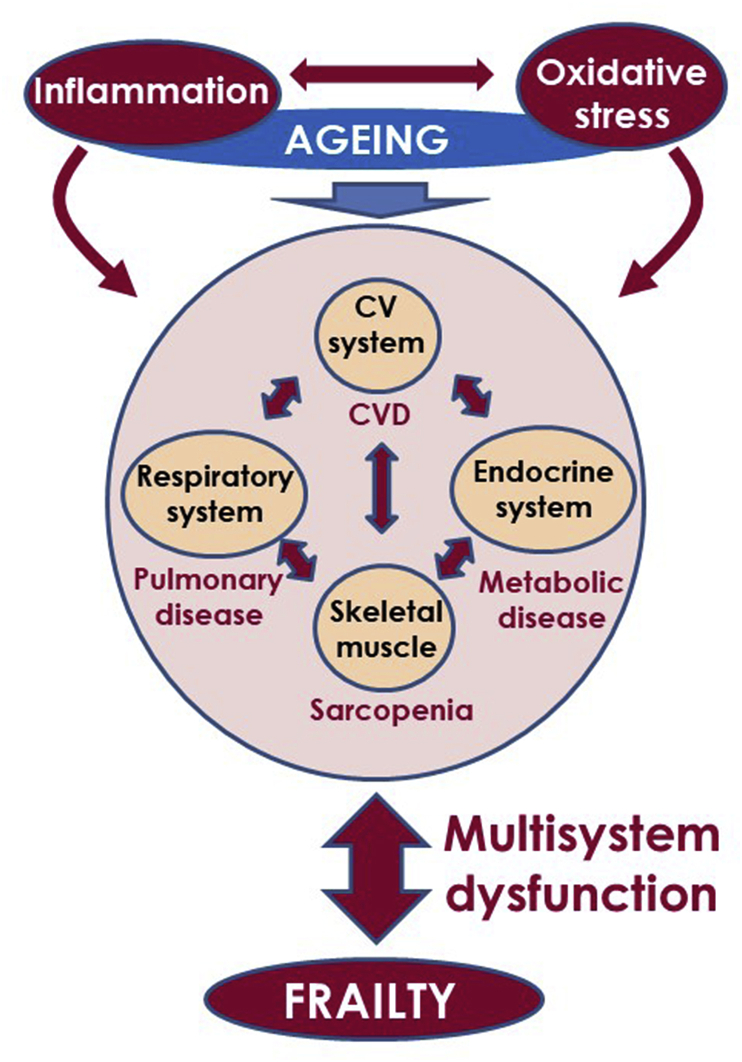
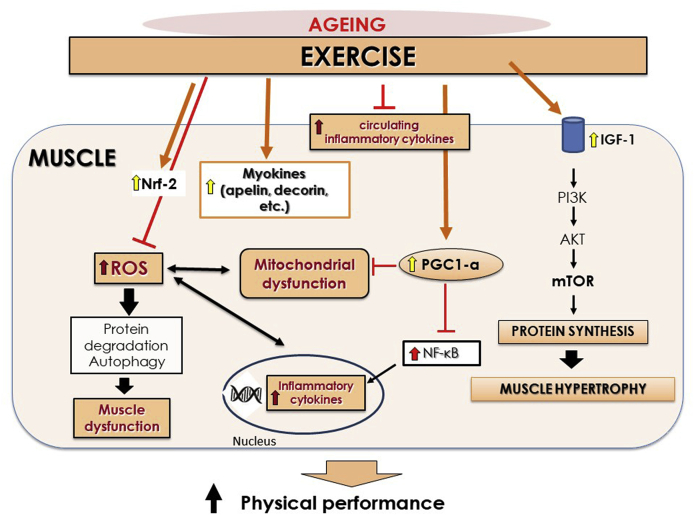
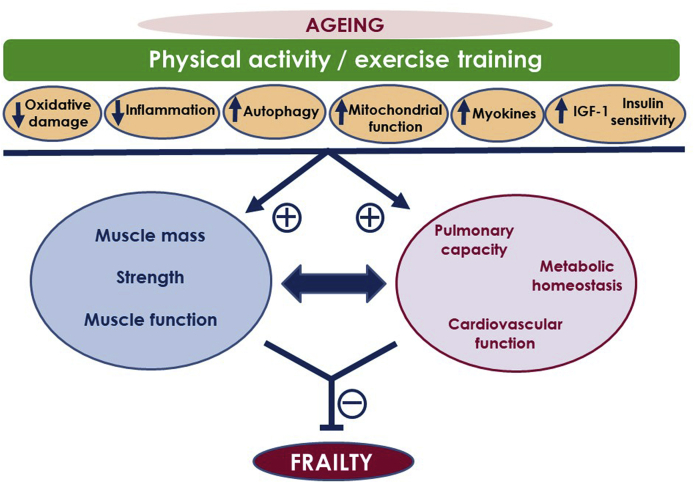
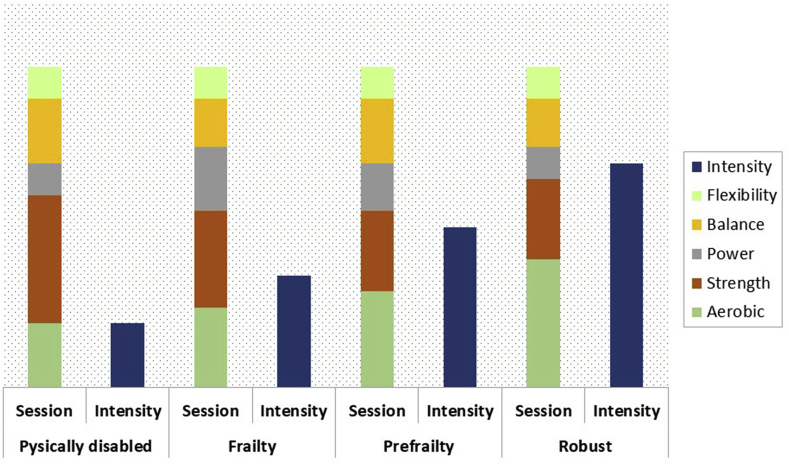
Frailty, a consequence of the interaction of the aging process and certain chronic diseases, compromises functional outcomes in the elderly and substantially increases their risk for developing disabilities and other adverse outcomes. Frailty follows from the combination of several impaired physiological mechanisms affecting multiple organs and systems. And, though frailty and sarcopenia are related, they are two different conditions. Thus, strategies to preserve or improve functional status should consider systemic function in addition to muscle conditioning. Physical activity/exercise is considered one of the main strategies to counteract frailty-related physical impairment in the elderly. Exercise reduces age-related oxidative damage and chronic inflammation, increases autophagy, and improves mitochondrial function, myokine profile, insulin-like growth factor-1 (IGF-1) signaling pathway, and insulin sensitivity. Exercise interventions target resistance (strength and power), aerobic, balance, and flexibility work. Each type improves different aspects of physical functioning, though they could be combined according to need and prescribed as a multicomponent intervention. Therefore, exercise intervention programs should be prescribed based on an individual's physical functioning and adapted to the ensuing response.
Keywords: Aging; Exercise; Frailty; Multicomponent intervention; Oxidative stress; Physical activity.
Copyright © 2020. Published by Elsevier B.V.
Conflict of interest statement
Declaration of competing interest No Conflicts Of Interest.
Figures
References
-
- Dzau V.J., Inouye S.K., Rowe J.W., Finkelman E., Yamada T. Enabling healthful aging for all. The National Academy of Medicine grand challenge in health longevity. N. Engl. J. Med. 2019;381:1699–1701. - PubMed
-
- He W., Goodkind D., Kowal P. U.S. Government Publishing Office; Washington, DC: 2016. U.S. Census Bureau, International Population Reports, P95/16-1, an Aging World: 2015.
-
- Hayflick L. The not-so-close relationship between biological aging and age-associated pathologies in humans. J Gerontol A Biol Sci Med Sci. 2004;59:B547–B550. - PubMed
-
- Hayflick L. Biological aging is no longer an unsolved problem. Ann. N. Y. Acad. Sci. 2007;1100:1–13. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
