

Assessing efficacy of CytoSorb haemoadsorber for prevention of organ dysfunction in cardiac surgery patients with infective endocarditis: REMOVE-protocol for randomised controlled trial
- PMID: 32234739
- PMCID: PMC7170567
- DOI: 10.1136/bmjopen-2019-031912
Assessing efficacy of CytoSorb haemoadsorber for prevention of organ dysfunction in cardiac surgery patients with infective endocarditis: REMOVE-protocol for randomised controlled trial
Abstract
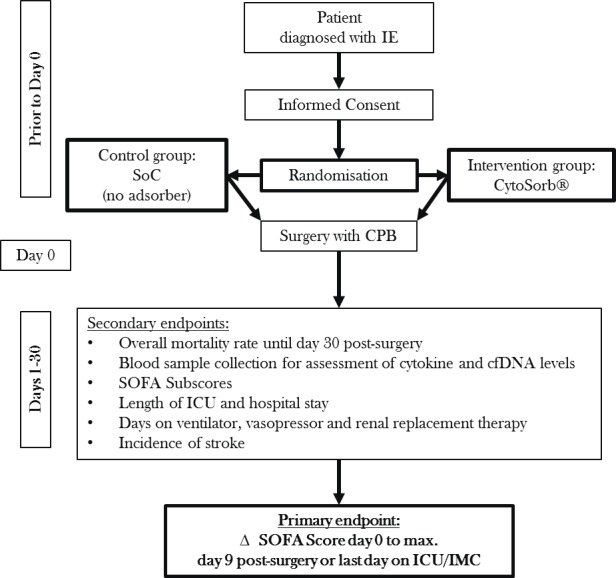
Introduction: Infective endocarditis (IE) is associated with high mortality and morbidity. Multiple organ failure is the main cause of death after surgery for IE. Cardiopulmonary bypass (CPB) can cause a systemic inflammatory response. In a pilot study (REMOVE-pilot (Revealing mechanisms and investigating efficacy of hemoad-sorption for prevention of vasodilatory shock in cardiac surgery patients with infective endocarditis - a multicentric randomized controlled group sequential trial)), we found that plasma profiles of cytokines during and after CPB were higher in patients with IE compared with patients with non-infectious valvular heart disease. Sequential Organ Failure Assessment (SOFA) scores on the first and second postoperative days and in-hospital mortality were also higher in IE patients. This protocol describes the design of the REMOVE trial on cytokine-adsorbing columns, for example, CytoSorb, for non-selective removal of cytokines. The aim of the REMOVE study is to demonstrate efficacy of CytoSorb on the prevention of multiorgan dysfunction in patients with IE undergoing cardiac surgery.
Methods and analysis: The REMOVE study is an interventional randomised controlled multicenter trial with a group sequential (Pocock) design for assessing efficacy of CytoSorb in patients undergoing cardiac surgery for IE. The change in mean total SOFA (∆ SOFA) score between preoperative and postoperative care will be used as primary endpoint. Data on 30-day mortality, changes in cytokines levels, duration of mechanical ventilation, length of intensive care unit and hospital stay, and postoperative stroke will be collected as secondary endpoints. An interim analysis will be conducted after including 25 participating patients per study arm (with a focus on feasibility of the recruitment as well as differences in cytokines and cell-free DNA levels).
Ethics and dissemination: The protocol was approved by the institutional review board and ethics committee of the University of Jena as well as by the corresponding ethics committee of each participating study centre. The results will be published in a renowned international medical journal, irrespective of the outcomes of the study.
Trial registration number: The ClinicalTrials.gov registry (NCT03266302).
Keywords: cardiac surgery; cytokines; cytosorb®; hemoadsorption; infective endocarditis; organ dysfunction.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: FMB reports grants and personal fees from CytoSorbents Europe,outside the submitted work.
Figures

References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical