

Center-level Variation in HLA-incompatible Living Donor Kidney Transplantation Outcomes
- PMID: 32235255
- PMCID: PMC8080262
- DOI: 10.1097/TP.0000000000003254
Center-level Variation in HLA-incompatible Living Donor Kidney Transplantation Outcomes
Abstract
Background: Desensitization protocols for HLA-incompatible living donor kidney transplantation (ILDKT) vary across centers. The impact of these, as well as other practice variations, on ILDKT outcomes remains unknown.
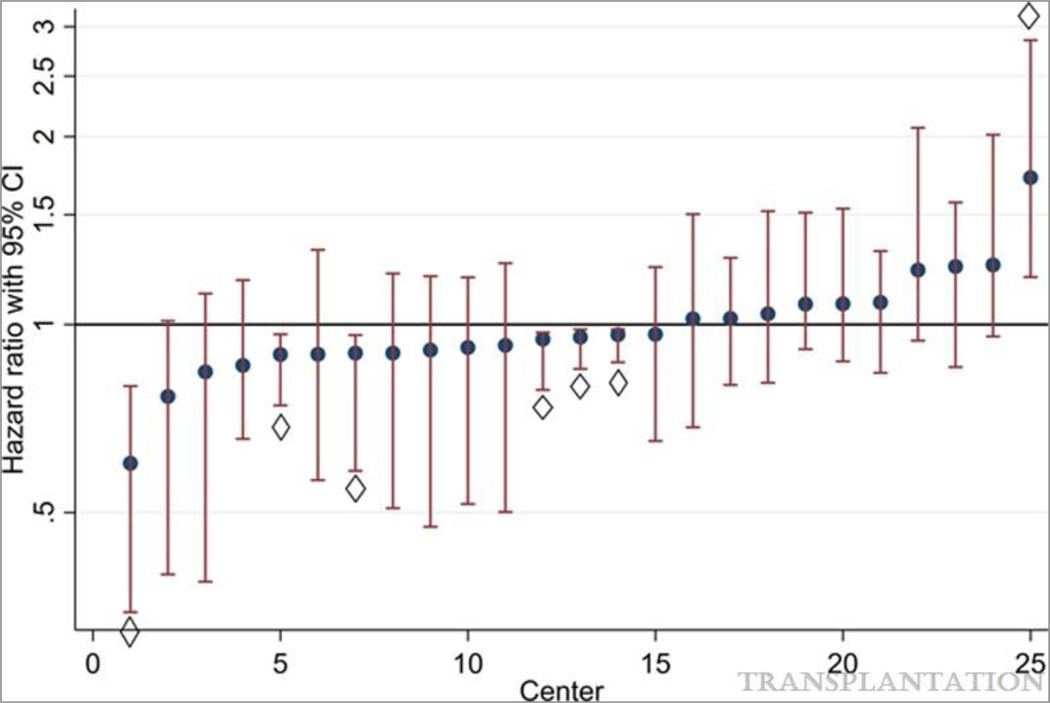
Methods: We sought to quantify center-level variation in mortality and graft loss following ILDKT using a 25-center cohort of 1358 ILDKT recipients with linkage to Scientific Registry of Transplant Recipients for accurate outcome ascertainment. We used multilevel Cox regression with shared frailty to determine the variation in post-ILDKT outcomes attributable to between-center differences and to identify any center-level characteristics associated with improved post-ILDKT outcomes.
Results: After adjusting for patient-level characteristics, only 6 centers (24%) had lower mortality and 1 (4%) had higher mortality than average. Similarly, only 5 centers (20%) had higher graft loss and 2 had lower graft loss than average. Only 4.7% of the differences in mortality (P < 0.01) and 4.4% of the differences in graft loss (P < 0.01) were attributable to between-center variation. These translated to a median hazard ratio of 1.36 for mortality and 1.34 of graft loss for similar candidates at different centers. Post-ILDKT outcomes were not associated with the following center-level characteristics: ILDKT volume and transplanting a higher proportion of highly sensitized, prior transplant, preemptive, or minority candidates.
Conclusions: Unlike most aspects of transplantation in which center-level variation and volume impact outcomes, we did not find substantial evidence for this in ILDKT. Our findings support the continued practice of ILDKT across these diverse centers.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

References
-
- Montgomery RA, Lonze BE, King KE, et al. Desensitization in HLA-Incompatible Kidney Recipients and Survival. New England Journal of Medicine. 2011;365(4): 318–326. - PubMed
-
- Montgomery RA, Lonze BE, Jackson AM. Using donor exchange paradigms with desensitization to enhance transplant rates among highly sensitized patients. Curr Opin Organ Transplant. 2011;16(4): 439–443. - PubMed
-
- Montgomery RA. Renal Transplantation Across HLA and ABO Antibody Barriers: Integrating Paired Donation into Desensitization Protocols. American Journal of Transplantation. 2010;10(3): 449–457. - PubMed
-
- Jordan SC, Choi J, Vo A. Kidney transplantation in highly sensitized patients. Br Med Bull. 2015;114(1): 113–125. - PubMed
