

Immunotherapy in Glioblastoma: Current Shortcomings and Future Perspectives
- PMID: 32235752
- PMCID: PMC7140029
- DOI: 10.3390/cancers12030751
Immunotherapy in Glioblastoma: Current Shortcomings and Future Perspectives
Abstract
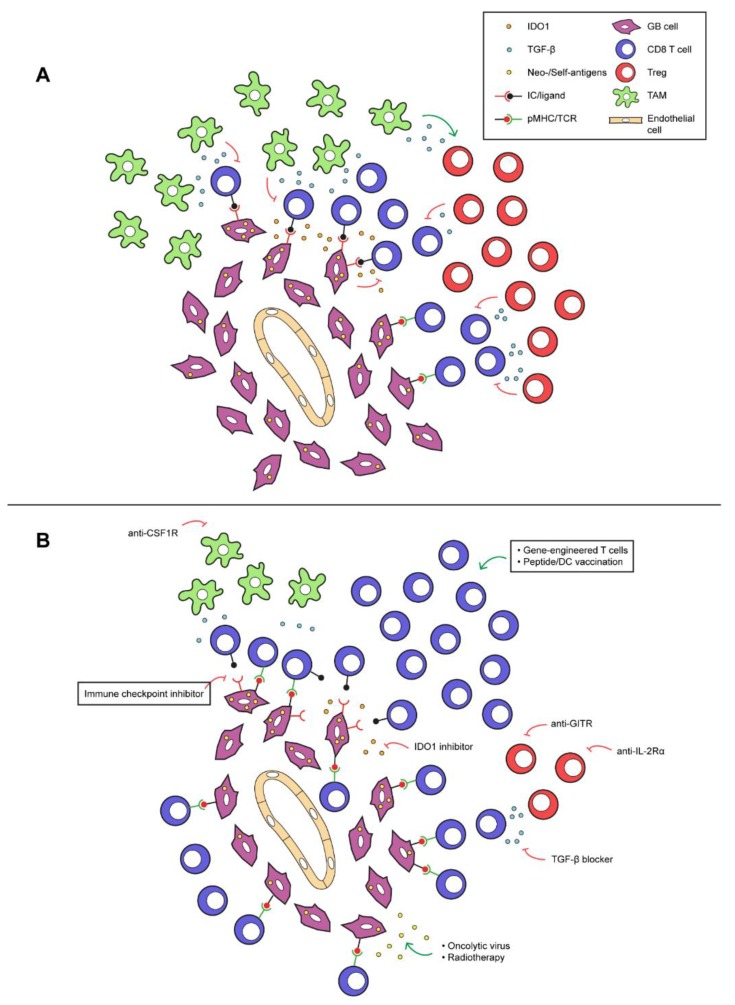
Glioblastomas are aggressive, fast-growing primary brain tumors. After standard-of-care treatment with radiation in combination with temozolomide, the overall prognosis of newly diagnosed patients remains poor, with a 2-year survival rate of less than 20%. The remarkable survival benefit gained with immunotherapy in several extracranial tumor types spurred a variety of experimental intervention studies in glioblastoma patients. These ranged from immune checkpoint inhibition to vaccinations and adoptive T cell therapies. Unfortunately, almost all clinical outcomes were universally disappointing. In this perspective, we provide an overview of immune interventions performed to date in glioblastoma patients and re-evaluate their performance. We argue that shortcomings of current immune therapies in glioblastoma are related to three major determinants of resistance, namely: low immunogenicity; immune privilege of the central nervous system; and immunosuppressive micro-environment. In this perspective, we propose strategies that are guided by exact shortcomings to sensitize glioblastoma prior to treatment with therapies that enhance numbers and/or activation state of CD8 T cells.
Keywords: adoptive T cell therapy; antigens; checkpoint inhibitors; clinical studies; glioblastoma; immune privilege; tumor micro-environment; vaccines.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ostrom Q.T., Gittleman H., Liao P., Vecchione-Koval T., Wolinsky Y., Kruchko C., Barnholtz-Sloan J.S. Cbtrus statistical report: Primary brain and other central nervous system tumors diagnosed in the united states in 2010–2014. Neuro. Oncol. 2017;19:v1–v88. doi: 10.1093/neuonc/nox158. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
