

Antioxidant Therapies in Traumatic Brain Injury
- PMID: 32235799
- PMCID: PMC7139349
- DOI: 10.3390/antiox9030260
Antioxidant Therapies in Traumatic Brain Injury
Abstract
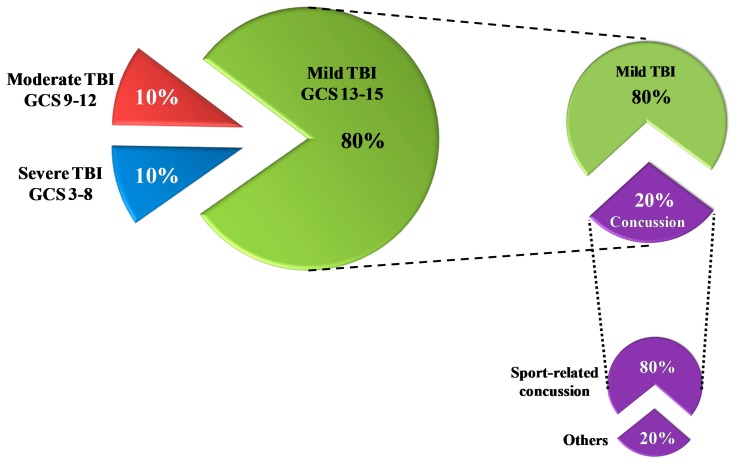
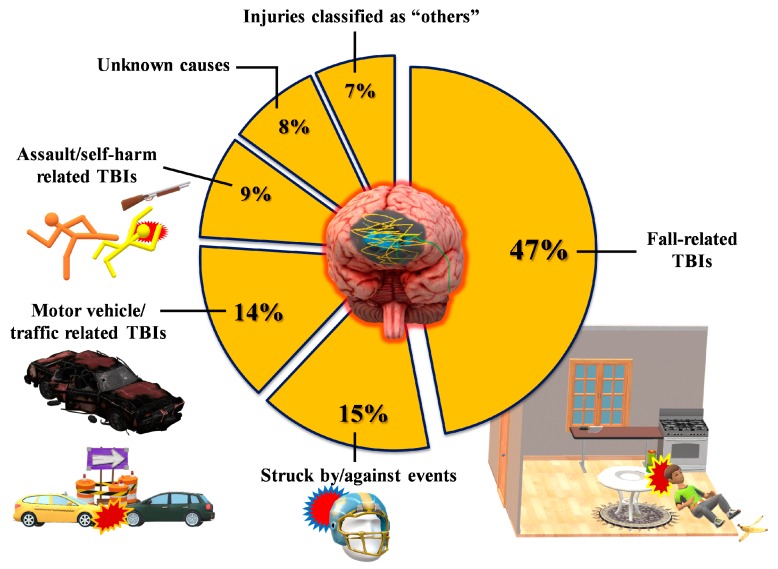
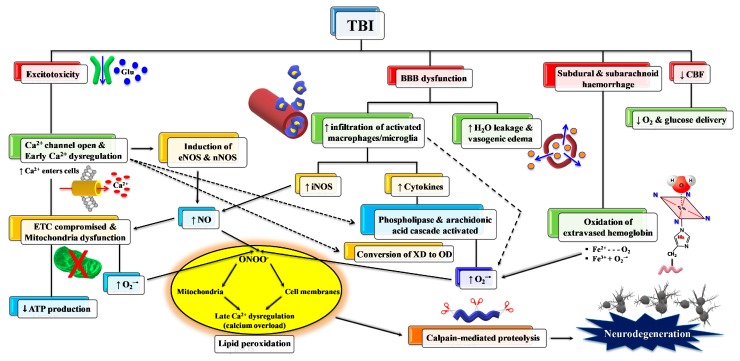
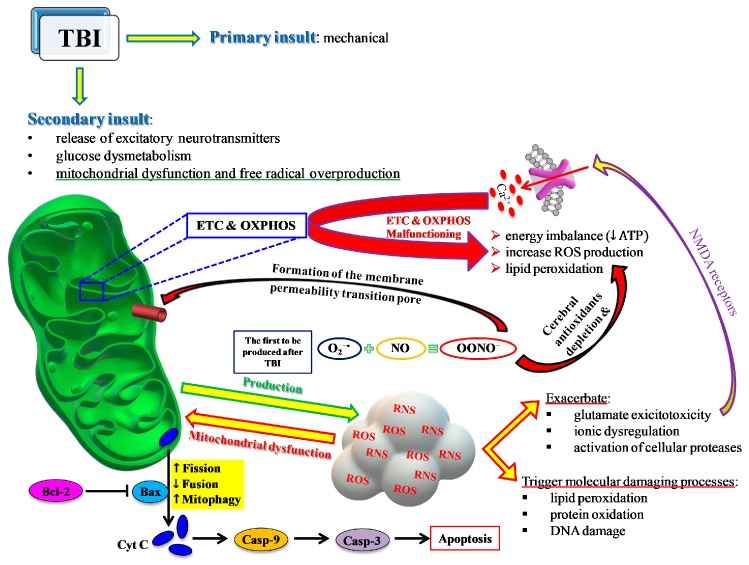
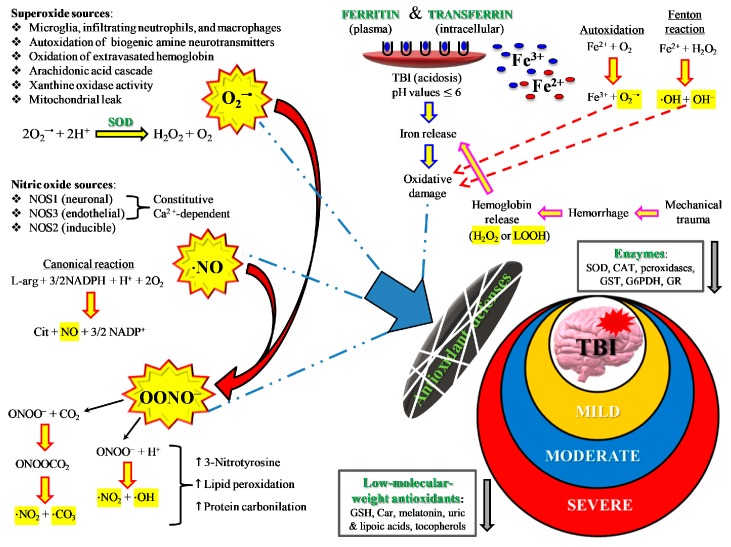
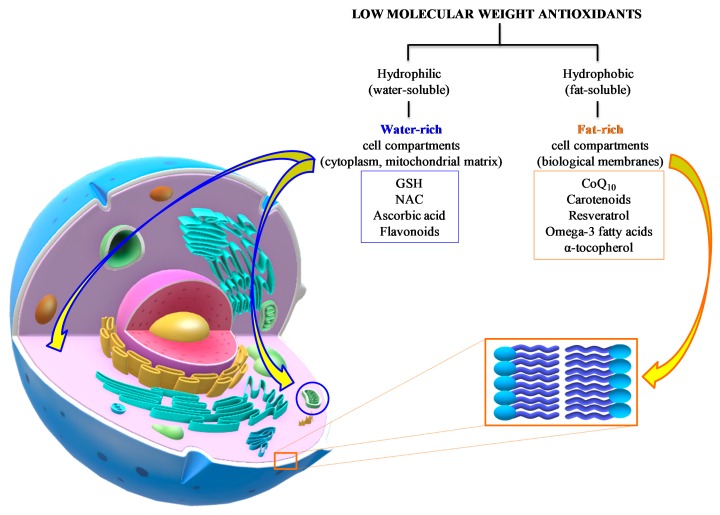
Due to a multiplicity of causes provoking traumatic brain injury (TBI), TBI is a highly heterogeneous pathology, characterized by high mortality and disability rates. TBI is an acute neurodegenerative event, potentially and unpredictably evolving into sub-chronic and chronic neurodegenerative events, with transient or permanent neurologic, cognitive, and motor deficits, for which no valid standardized therapies are available. A vast body of literature demonstrates that TBI-induced oxidative/nitrosative stress is involved in the development of both acute and chronic neurodegenerative disorders. Cellular defenses against this phenomenon are largely dependent on low molecular weight antioxidants, most of which are consumed with diet or as nutraceutical supplements. A large number of studies have evaluated the efficacy of antioxidant administration to decrease TBI-associated damage in various animal TBI models and in a limited number of clinical trials. Points of weakness of preclinical studies are represented by the large variability in the TBI model adopted, in the antioxidant tested, in the timing, dosages, and routes of administration used, and in the variety of molecular and/or neurocognitive parameters evaluated. The analysis of the very few clinical studies does not allow strong conclusions to be drawn on the real effectiveness of antioxidant administration to TBI patients. Standardizing TBI models and different experimental conditions, as well as testing the efficacy of administration of a cocktail of antioxidants rather than only one, should be mandatory. According to some promising clinical results, it appears that sports-related concussion is probably the best type of TBI to test the benefits of antioxidant administration.
Keywords: concussion; low molecular weight antioxidants; oxidative/nitrosative stress; traumatic brain injury.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Maas A.I.R., Menon D.K., Adelson P.D., Andelic N., Bell M.J., Belli A., Bragge P., Brazinova A., Buki A., Chesnut R.M., et al. InTBIR Participants and Investigators. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017;16:987–1048. doi: 10.1016/S1474-4422(17)30371-X. - DOI - PubMed
-
- World Health Oraganization Neurological Disorders: Public Health Challenges. [(accessed on 19 July 2019)];2006 Available online: https://www.who.int/mental_health/neurology/chapter_3_b_neuro_disorders_....
-
- Carroll L.J., Cassidy J.D., Holm L., Kraus J., Coronado V.G. WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Methodological issues and research recommendations for mild traumatic brain injury: The WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J. Rehabil. Med. 2004;43:113–125. doi: 10.1080/16501960410023877. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
