

Relationship between serum calcium or phosphate levels and mortality stratified by parathyroid hormone level: an analysis from the MBD-5D study
- PMID: 32236781
- PMCID: PMC7271007
- DOI: 10.1007/s10157-020-01879-8
Relationship between serum calcium or phosphate levels and mortality stratified by parathyroid hormone level: an analysis from the MBD-5D study
Abstract
Introduction: There is limited evidence about the association between calcium and phosphate levels and mortality stratified by intact parathyroid hormone (iPTH) level.
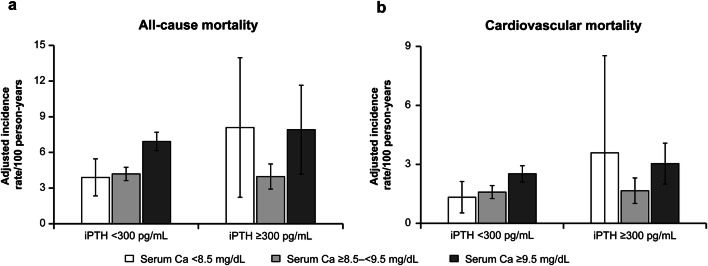
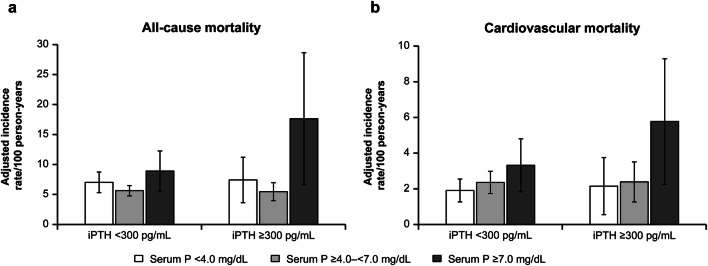
Methods: We investigated whether differences in iPTH level affect the relationship between calcium and phosphate levels and all-cause mortality in hemodialysis patients with secondary hyperparathyroidism (SHPT). Calcium and phosphate levels were categorized as low (< 8.5 mg/dL, < 4.0 mg/dL), medium (≥ 8.5-< 9.5 mg/dL, ≥ 4.0-< 7.0 mg/dL), and high (≥ 9.5 mg/dL, ≥ 7.0 mg/dL), respectively. iPTH levels were grouped into < 300 or ≥ 300 pg/mL. Adjusted incidence rate ratios (aIRRs) were analyzed by weighted Poisson regression.
Results: For calcium, patients with higher iPTH (≥ 300 pg/mL) had significantly higher all-cause mortality rates in the high than in the medium category (aIRR 1.99, 95% confidence interval [CI] 1.16-3.42), and tended to have a higher mortality rate in the low category (aIRR 2.04, 95% CI 0.94-4.42). Patients with lower iPTH (< 300 pg/mL) had higher mortality rates in the high than in the medium category (aIRR 1.65, 95% CI 1.39-1.96). For phosphate, the mortality rate was significantly higher in the high than in the medium category in patients with higher and lower iPTH (aIRR 3.23, 95% CI 1.63-6.39 for iPTH ≥ 300 pg/mL; aIRR 1.58, 95% CI 1.06-2.36 for iPTH < 300 pg/mL).
Conclusion: High calcium and phosphate levels were associated with increased risk of mortality irrespective of iPTH level.
Keywords: Calcium; Chronic kidney disease–mineral and bone disorder; Hemodialysis; Mortality; Parathyroid hormone; Phosphate.
Conflict of interest statement
SA, YE, TN, and MW are employees of Kyowa Kirin Co., Ltd. (KKC). KY has received consulting fees from Torii Pharmaceutical, and lecture fees from KKC, Torii Pharmaceutical, and Ono Pharmaceutical. CM and YO do not have any conflicts of interest to declare. S. Fukuma has acted as a scientific advisor for KKC. MF has received consulting fees from KKC and Ono Pharmaceutical; lecture fees from KKC, Bayer, Torii Pharmaceutical, and Ono Pharmaceutical; and grants from KKC and Bayer. S. Fukuhara has acted as a scientific advisor for and has received grants from KKC. TA has received consulting fees from KKC, Astellas Pharma, Bayer, Fuso Pharmaceutical, Japan Tobacco, Ono Pharmaceutical, Sanwa Chemical, Otsuka, GSK and NIPRO, and lecture fees from KKC, Chugai Pharmaceutical, Bayer, Kissei Pharmaceutical, Torii Pharmaceutical, and Ono Pharmaceutical.
Figures
References
-
- Tentori F, Blayney MJ, Albert JM, Gillespie BW, Kerr PG, Bommer J, et al. Mortality risk for dialysis patients with different levels of serum calcium, phosphorus, and PTH: the Dialysis Outcomes and Practice Patterns Study (DOPPS) Am J Kidney Dis. 2008;52:519–530. doi: 10.1053/j.ajkd.2008.03.020. - DOI - PubMed
