

Effect of Delayed Targeted Intraoperative Radiotherapy vs Whole-Breast Radiotherapy on Local Recurrence and Survival: Long-term Results From the TARGIT-A Randomized Clinical Trial in Early Breast Cancer
- PMID: 32239210
- PMCID: PMC7348682
- DOI: 10.1001/jamaoncol.2020.0249
Effect of Delayed Targeted Intraoperative Radiotherapy vs Whole-Breast Radiotherapy on Local Recurrence and Survival: Long-term Results From the TARGIT-A Randomized Clinical Trial in Early Breast Cancer
Erratum in
-
Change in License Type and Error in Figure 1.JAMA Oncol. 2020 Jul 1;6(7):1123. doi: 10.1001/jamaoncol.2020.1749. JAMA Oncol. 2020. PMID: 32437501 Free PMC article. No abstract available.
Abstract
Importance: Conventional adjuvant radiotherapy for breast cancer given daily for several weeks is onerous and expensive. Some patients may be obliged to choose a mastectomy instead, and some may forgo radiotherapy altogether. We proposed a clinical trial to test whether radiotherapy could be safely limited to the tumor bed.
Objective: To determine whether delayed second-procedure targeted intraoperative radiotherapy (TARGIT-IORT) is noninferior to whole-breast external beam radiotherapy (EBRT) in terms of local control.
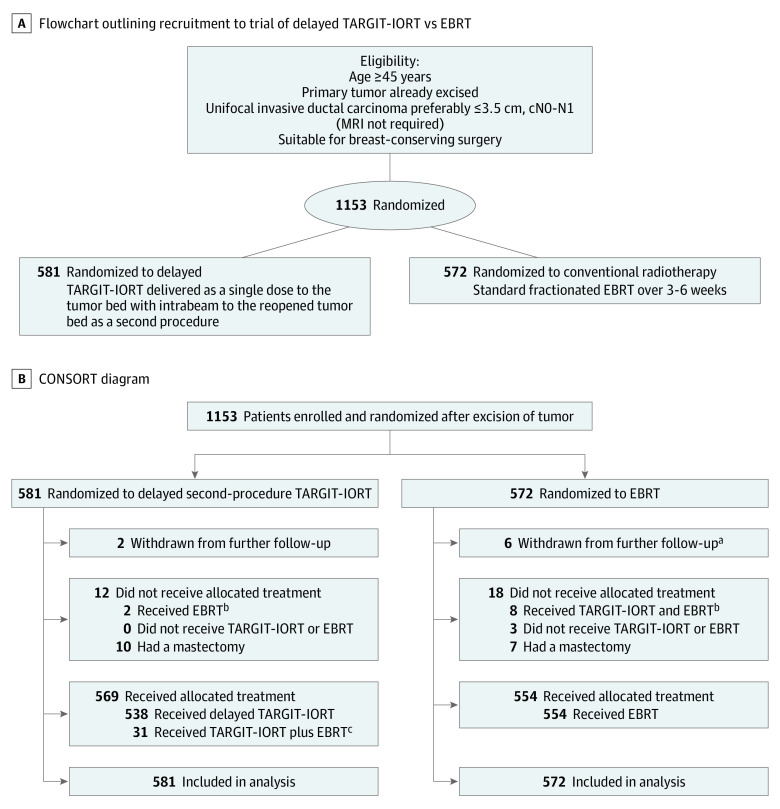
Design, setting, and participants: In this prospective, randomized (1:1 ratio) noninferiority trial, 1153 patients aged 45 years or older with invasive ductal breast carcinoma smaller than 3.5 cm treated with breast conservation were enrolled from 28 centers in 9 countries. Data were locked in on July 3, 2019.
Interventions: The TARGIT-A trial was started in March 2000; patients were randomized after needle biopsy to receive TARGIT-IORT immediately after lumpectomy under the same anesthetic vs EBRT and results have been shown to be noninferior. A parallel study, described in this article, was initiated in 2004; patients who had their cancer excised were randomly allocated using separate randomization tables to receive EBRT or delayed TARGIT-IORT given as a second procedure by reopening the lumpectomy wound.
Main outcomes and measures: A noninferiority margin for local recurrence rate of 2.5% at 5 years, and long-term survival outcomes.
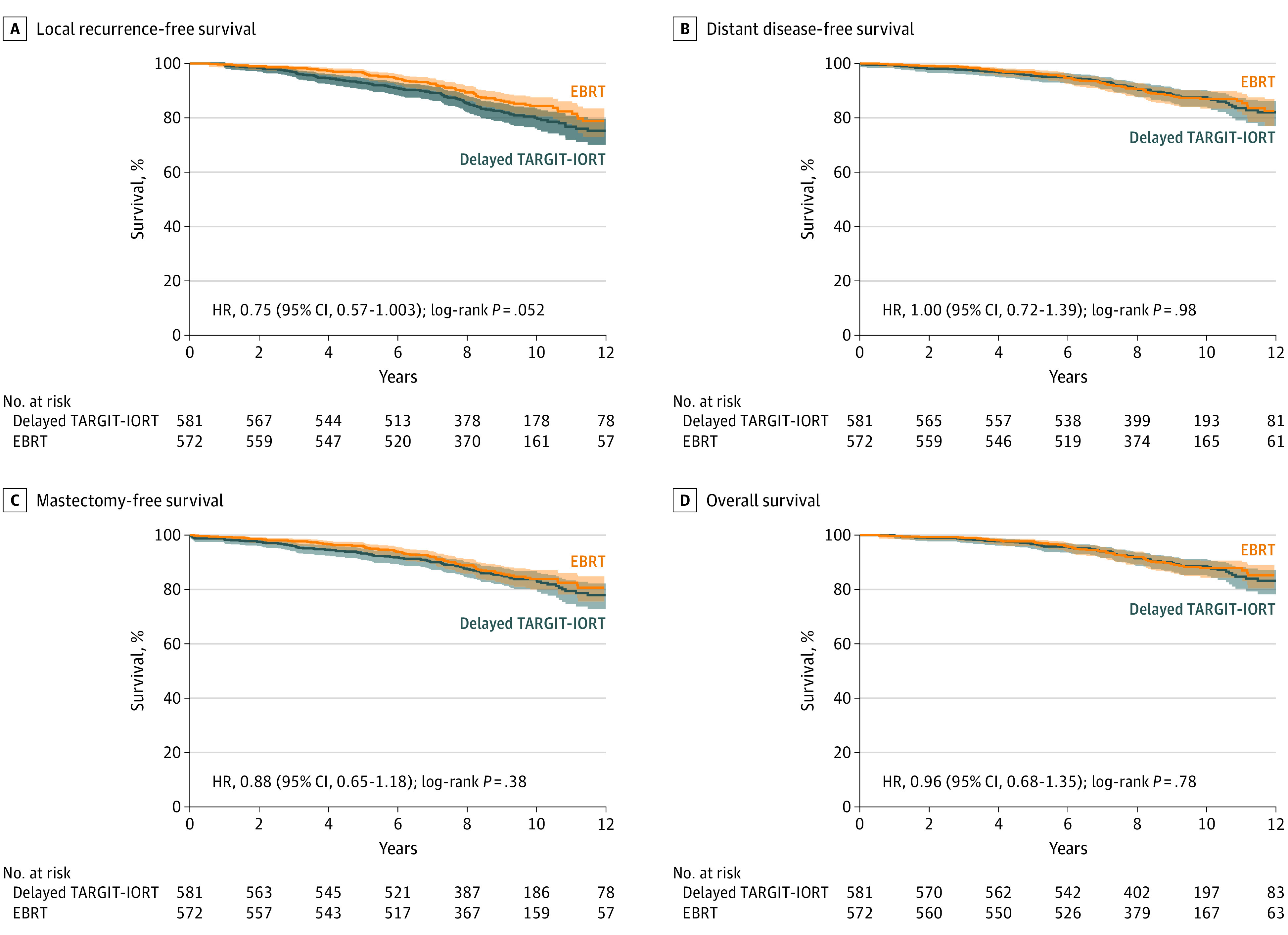
Results: Overall, 581 women (mean [SD] age, 63 [7] years) were randomized to delayed TARGIT-IORT and 572 patients (mean [SD] age, 63 [8] years) were randomized to EBRT. Sixty patients (5%) had tumors larger than 2 cm, or had positive nodes and only 32 (2.7%) were younger than 50 years. Delayed TARGIT-IORT was not noninferior to EBRT. The local recurrence rates at 5-year complete follow-up were: delayed TARGIT-IORT vs EBRT (23/581 [3.96%] vs 6/572 [1.05%], respectively; difference, 2.91%; upper 90% CI, 4.4%). With long-term follow-up (median [IQR], 9.0 [7.5-10.5] years), there was no statistically significant difference in local recurrence-free survival (HR, 0.75; 95% CI, 0.57-1.003; P = .052), mastectomy-free survival (HR, 0.88; 95% CI, 0.65-1.18; P = .38), distant disease-free survival (HR, 1.00; 95% CI, 0.72-1.39; P = .98), or overall survival (HR, 0.96; 95% CI, 0.68-1.35; P = .80).
Conclusions and relevance: These long-term data show that despite an increase in the number of local recurrences with delayed TARGIT-IORT, there was no statistically significant decrease in mastectomy-free survival, distant disease-free survival, or overall survival.
Trial registration: ISRCTN34086741, ClinicalTrials.gov Identifier: NCT00983684.
Conflict of interest statement
Figures
Comment in
-
Targeted Intraoperative Radiotherapy for Early Breast Cancer.JAMA Oncol. 2020 Oct 1;6(10):1636-1637. doi: 10.1001/jamaoncol.2020.2719. JAMA Oncol. 2020. PMID: 32789481 No abstract available.
-
Targeted Intraoperative Radiotherapy for Early Breast Cancer-Reply.JAMA Oncol. 2020 Oct 1;6(10):1637-1638. doi: 10.1001/jamaoncol.2020.2730. JAMA Oncol. 2020. PMID: 32789486 No abstract available.
-
Targeted Intraoperative Radiotherapy for Early Breast Cancer.JAMA Oncol. 2020 Oct 1;6(10):1635-1636. doi: 10.1001/jamaoncol.2020.2713. JAMA Oncol. 2020. PMID: 32789499 No abstract available.
-
Targeted Intraoperative Radiotherapy for Early Breast Cancer.JAMA Oncol. 2020 Oct 1;6(10):1636. doi: 10.1001/jamaoncol.2020.2716. JAMA Oncol. 2020. PMID: 32789502 No abstract available.
References
-
- Vaidya JS, Baum M, Tobias JS, Houghton J Targeted Intraoperative Radiothearpy (TARGIT)- trial protocol. Lancet. 1999; https://www.thelancet.com/protocol-reviews/99PRT-47.
-
- Vaidya JS. A novel approach for local treatment of early breast cancer. PhD Thesis, University College London, University of London 2002. https://www.ucl.ac.uk/~rmhkjsv/papers/thesis.htm. Accessed November 9, 2019.
