

Association of Organizational Factors and Physician Practices' Participation in Alternative Payment Models
- PMID: 32239223
- PMCID: PMC7118519
- DOI: 10.1001/jamanetworkopen.2020.2019
Association of Organizational Factors and Physician Practices' Participation in Alternative Payment Models
Abstract
Importance: Consolidation among physician practices and between hospitals and physician practices has accelerated in the past decade, resulting in higher prices in commercial markets. The resulting integration of health care across clinicians and participation in alternative payment models (APMs), which aim to improve quality while constraining spending, are cited as reasons for consolidation, but little is known about the association between integration and APM participation.
Objective: To examine the association of organizational characteristics, ownership, and integration with intensity of participation in APMs among physician practices.
Design, setting, and participants: A cross-sectional descriptive study, adjusted for sampling and nonresponse weights, was conducted in US physician practice respondents to the National Survey of Healthcare Organizations and Systems conducted between June 16, 2017, and August 17, 2018; of 2333 responses received (response rate, 46.9%) and after exclusion of ineligible and incomplete responses, the number of practices included in the analysis was 2061. Data analysis was performed from April 1, 2019, to August 31, 2019.
Exposures: Self-reported physician practice characteristics, including ownership, integration (clinical, cultural, financial, and functional), care delivery capabilities, activities, and environmental factors.
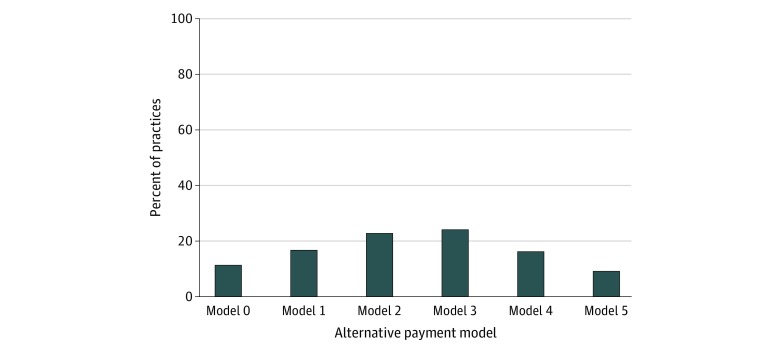
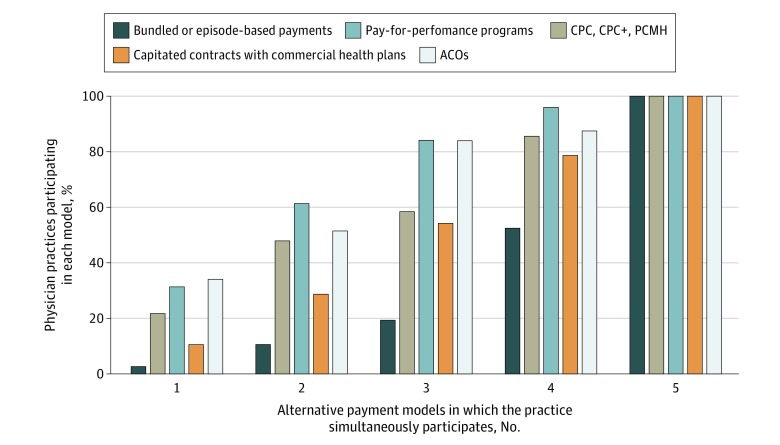
Main outcomes and measures: Participation in APMs: (1) bundled payments, (2) comprehensive primary care and medical home programs, (3) pay-for-performance programs, (4) capitated contracts with commercial health plans, and (5) accountable care organization contracts.
Results: A total of 49.2% of the 2061 practices included reported participating in 3 or more APMs; most participated in pay-for-performance and accountable care organization models. Covariate-adjusted analyses suggested that operating within a health care system (odds ratio [OR] for medical group: 2.35; 95% CI, 1.70-3.25; P < .001; simple health system: 1.46; 95% CI, 1.08-1.97; P = .02; and complex health system: 1.76; 95% CI, 1.25-2.47; P = .001 relative to independent practices), greater clinical (OR, 4.68; 95% CI, 2.28-9.59; P < .001) and functional (OR, 4.24; 95% CI, 2.00-8.97; P < .001) integration, and being located in the Northeast (OR for Midwest: 0.47; 95% CI, 0.34-0.65; P < .001; South: 0.47; 95% CI, 0.34-0.66; P < .001; and West: 0.64; 95% CI, 0.46-0.91; P = .01) were associated with greater APM participation.
Conclusions and relevance: Greater APM participation appears to be supported by integration and system ownership.
Figures
References
-
- Fuse Brown EC, King JS. The double-edged sword of health care integration: consolidation and cost control. Indiana Law J. 2016;92(1):2. doi:10.2139/ssrn.2736310 - DOI
-
- Shrank WH, Keyser D Diffusion of innovations in health care—obtaining evidence to move faster. Health Affairs blog. Vol 2018. Published May 16, 2017. Accessed March 2, 2020. https://www.healthaffairs.org/do/10.1377/hblog20170516.060078/full - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
