

Expediting clinician assessment in the diagnosis of autism spectrum disorder
- PMID: 32239502
- PMCID: PMC7540056
- DOI: 10.1111/dmcn.14530
Expediting clinician assessment in the diagnosis of autism spectrum disorder
Abstract
Aim: To investigate a novel observational rating protocol designed to expedite clinical diagnosis of autism spectrum disorder (ASD).
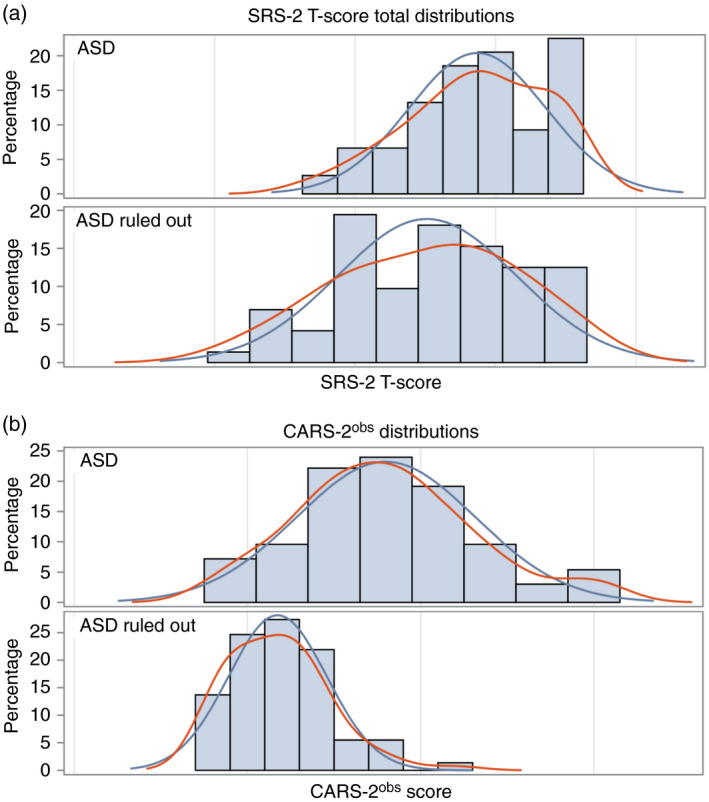
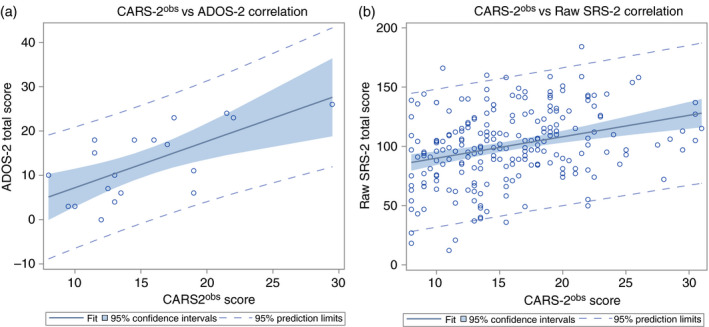
Method: Two hundred and forty patients referred to a tertiary autism center (median age 8y 9mo, range 2y 6mo-34y 8mo; 188 males, 52 females) were rated using an adaptation of the Childhood Autism Rating Scale, Second Edition (CARS-2) based exclusively on patient observation (CARS-2obs ). Scores were compared to expert diagnosis of ASD, parent-reported Social Responsiveness Scale, Second Edition (SRS-2) and, in a selected subset of patients, the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2).
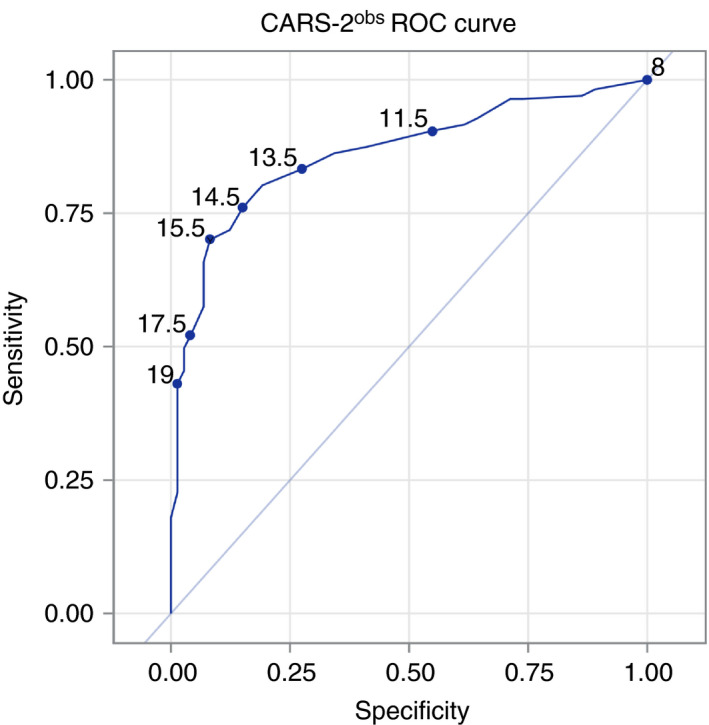
Results: CARS-2obs distinguished patients with a clinical diagnosis of ASD from those with non-ASD neuropsychiatric disorders (mean score=18 vs 11.7, p<0.001). Severity ratings on the CARS-2obs correlated with the ADOS-2 (r=0.68, ρ=0.64) and SRS-2 (r=0.31, ρ=0.32). A CARS-2obs cutoff point equal to or greater than 16 demonstrated 95.8% specificity and 62.3% sensitivity in discriminating individuals with ASD from individuals without ASD in a specialty referral setting.
Interpretation: The CARS-2obs allows the rapid acquisition of quantitative ratings of autistic severity by direct observation. Coupled with parent/teacher-reported symptoms and developmental history, the measure may contribute to a low-cost diagnostic paradigm in clinical and public health settings, where positive results might help reduce delays in diagnosis, and negative results could prompt further specialty assessment.
What this paper adds: The Childhood Autism Rating Scale, Second Edition based on patient observation distinguished individuals with versus without autism spectrum disorder (ASD). A score equal to or greater than 16 on this assessment showed high specificity for a diagnosis of ASD.
© 2020 Mac Keith Press.
Figures
Comment in
-
Proposed brief diagnostic observational scale for autism spectrum disorder.Dev Med Child Neurol. 2020 Jul;62(7):772. doi: 10.1111/dmcn.14531. Epub 2020 Mar 28. Dev Med Child Neurol. 2020. PMID: 32222044 No abstract available.
References
-
- Lichtenstein P, Carlström E, Råstam M, Gillberg C, Anckarsäter H. The genetics of autism spectrum disorders and related neuropsychiatric disorders in childhood. Am J Psychiatry 2010; 167: 1357–63. - PubMed
-
- Constantino JN, Charman T. Diagnosis of autism spectrum disorder: reconciling the syndrome, its diverse origins, and variation in expression. Lancet Neurol 2016; 15: 279–91. - PubMed
-
- Lord C, Rutter M, Le Couteur A. Autism diagnostic interview‐revised: a revised version of a diagnostic interview for carers of individuals with possible pervasive developmental disorders. J Autism Dev Disord 1994; 24: 659–85. - PubMed
-
- Lord C, Rutter M, DiLavore PC, Risi S. Autism Diagnostic Observation Schedule‐WPS (WPS edition). Los Angeles, CA: Western Psychological Services, 1999.
