

Applicability and reproducibility of acute myeloid leukaemia stem cell assessment in a multi-centre setting
- PMID: 32239670
- PMCID: PMC7540683
- DOI: 10.1111/bjh.16594
Applicability and reproducibility of acute myeloid leukaemia stem cell assessment in a multi-centre setting
Abstract
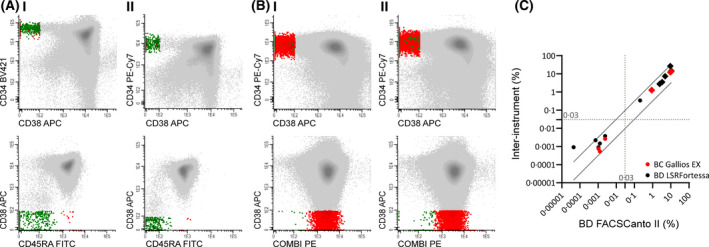
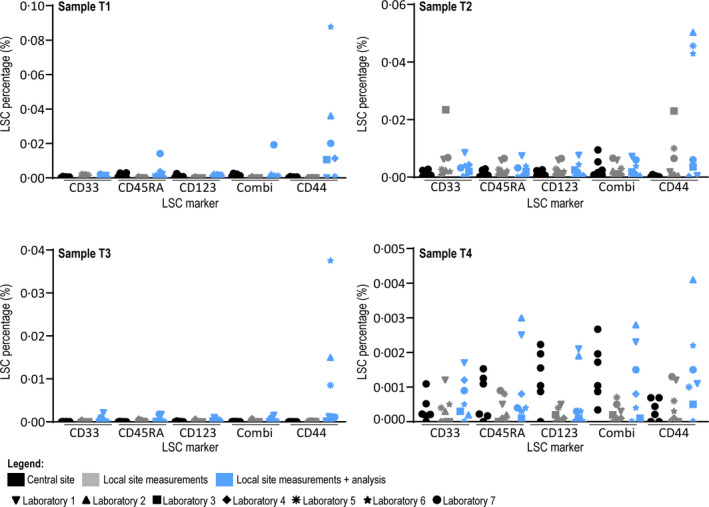
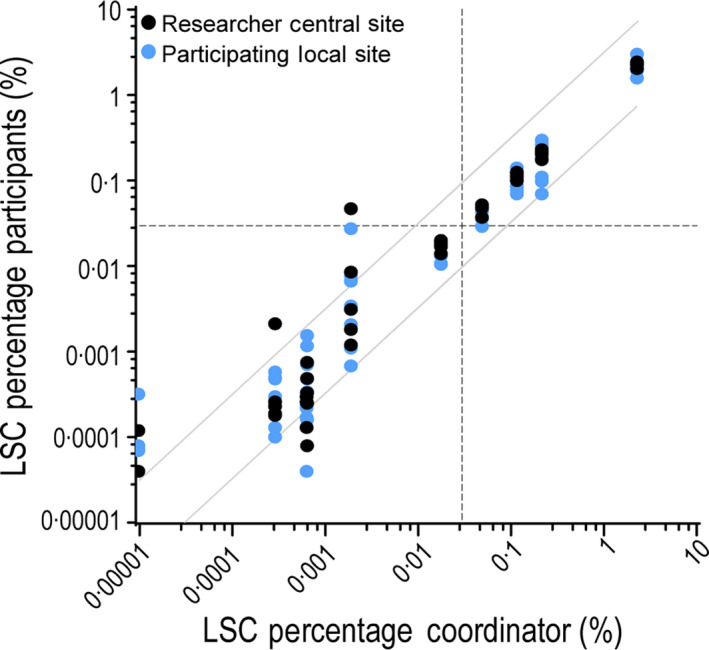
Leukaemic stem cells (LSC) have been experimentally defined as the leukaemia-propagating population and are thought to be the cellular reservoir of relapse in acute myeloid leukaemia (AML). Therefore, LSC measurements are warranted to facilitate accurate risk stratification. Previously, we published the composition of a one-tube flow cytometric assay, characterised by the presence of 13 important membrane markers for LSC detection. Here we present the validation experiments of the assay in several large AML research centres, both in Europe and the United States. Variability within instruments and sample processing showed high correlations between different instruments (Rpearson > 0·91, P < 0·001). Multi-centre testing introduced variation in reported LSC percentages but was found to be below the clinical relevant threshold. Clear gating protocols resulted in all laboratories being able to perform LSC assessment of the validation set. Participating centres were nearly unanimously able to distinguish LSChigh (>0·03% LSC) from LSClow (<0·03% LSC) despite inter-laboratory variation in reported LSC percentages. This study proves that the LSC assay is highly reproducible. These results together with the high prognostic impact of LSC load at diagnosis in AML patients render the one-tube LSC assessment a good marker for future risk classification.
© 2020 The Authors. British Journal of Haematology published by British Society for Haematology and John Wiley & Sons Ltd.
Conflict of interest statement
Financial support for part of this research has been received by BD Biosciences. A lyophilised version of the LSC tube is currently in production and will become available, with royalty payments for intellectual property rights to the VUmc.
Figures
References
-
- Döhner H, Estey E, Grimwade D, Amadori S, Appelbaum FR, Büchner T, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129:424–47. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27895058 [cited 2019 July 4]. - PMC - PubMed
-
- Jongen‐Lavrencic M, Grob T, Hanekamp D, Kavelaars FG, al Hinai A, Zeilemaker A, et al. Molecular Minimal Residual Disease in Acute Myeloid Leukemia. N Engl J Med. 2018;378(13):1189–99. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29601269 [cited 2019 July 4]. - PubMed
-
- Gupta PB, Chaffer CL, Weinberg RA. Cancer stem cells: mirage or reality? Nat Med. 2009;15:1010–2. Available from: http://papers3://publication/doi/10.1038/nm0909‐1010 [cited 2019 July 4]. - DOI - PubMed
-
- Gerber JM, Smith BD, Ngwang B, Zhang H, Vala MS, Morsberger L, et al. A clinically relevant population of leukemic CD34(+)CD38(−) cells in acute myeloid leukemia. Blood. 2012;119:3571–7. Available from: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3325044&tool=p... [cited 2019 July 4]. - PMC - PubMed
-
- van Rhenen A, Feller N, Kelder A, Westra A, Rombouts E, Zweegman S, et al. High stem cell frequency in acute myeloid leukemia at diagnosis predicts high minimal residual disease and poor survival. Clin Cancer Res. 2005;11:6520–7. Available from: http://clincancerres.aacrjournals.org/cgi/doi/10.1158/1078‐0432.CCR‐05‐0468 [cited 2019 July 4]. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
