

Neurosurgical Intervention for Supratentorial Intracerebral Hemorrhage
- PMID: 32239722
- PMCID: PMC7497162
- DOI: 10.1002/ana.25732
Neurosurgical Intervention for Supratentorial Intracerebral Hemorrhage
Abstract
Objective: The effect of surgical treatment for supratentorial spontaneous intracerebral hemorrhage (ICH) and whether it is modified by key baseline characteristics and timing remains uncertain.
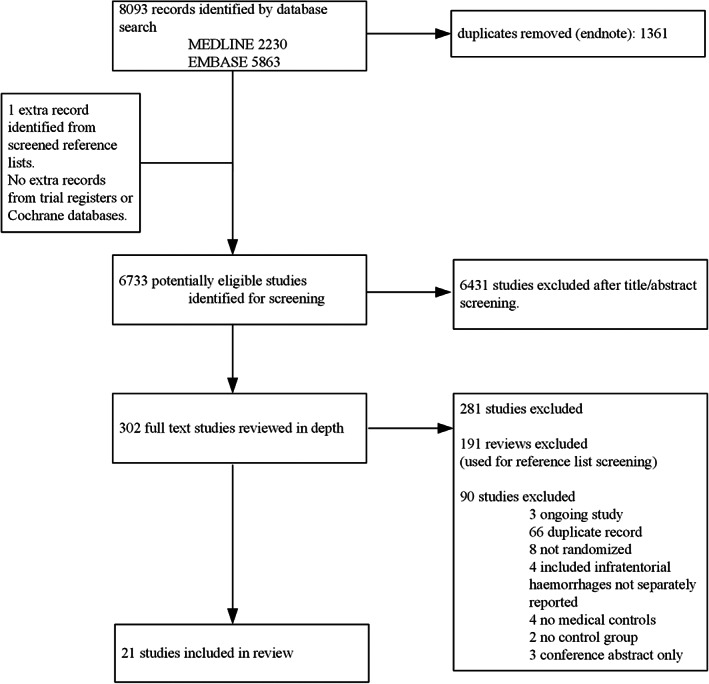
Methods: We performed a systematic review and meta-analysis of randomized controlled trials of surgical treatment of supratentorial spontaneous ICH aimed at clot removal. We searched MEDLINE, Embase, and Cochrane databases up to February 21, 2019. Primary outcome was good functional outcome at follow-up; secondary outcomes were death and serious adverse events. We analyzed all types of surgery combined and minimally invasive approaches separately. We pooled risk ratios with 95% confidence intervals and assessed the modifying effect of age, Glasgow Coma Scale, hematoma volume, and timing of surgery with meta-regression analysis.
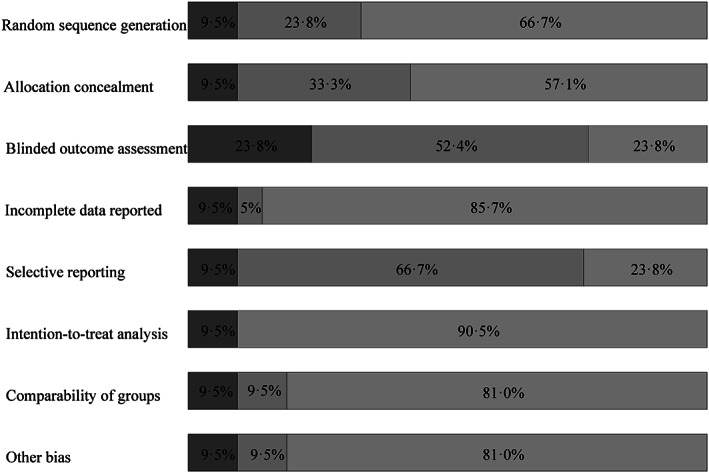
Results: We included 21 studies with 4,145 patients; 4 (19%) were of the highest quality. Risk ratio of good functional outcome after any type of surgery was 1.40 (95% confidence interval [CI] = 1.22-1.60, I2 = 46%, 20 studies), and after minimally invasive surgery it was 1.47 (95% CI = 1.26-1.72, I2 = 47%, 12 studies). For death, the risk ratio for any type of surgery was 0.77 (95% CI = 0.68-0.85, I2 = 23%, 21 studies), and for minimally invasive surgery it was 0.68 (95% CI = 0.56-0.83, I2 = 14%, 13 studies). Serious adverse events were reported infrequently. Surgery seemed more effective when performed sooner after symptom onset (p = 0.04, 12 studies). Age, Glasgow Coma Scale, and hematoma volume did not modify the effect of surgery.
Interpretation: Surgical treatment of supratentorial spontaneous ICH may be beneficial, in particular with minimally invasive procedures and when performed soon after symptom onset. Further well-designed randomized trials are needed to demonstrate whether (minimally invasive) surgery improves functional outcome after ICH and to determine the optimal time window of the treatment after symptom onset. ANN NEUROL 2020;88:239-250.
© 2020 The Authors. Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Figures





References
-
- Feigin VL, Lawes CM, Bennett DA, et al. Worldwide stroke incidence and early case fatality reported in 56 population‐based studies: a systematic review. Lancet Neurol 2009;8:355–369. - PubMed
-
- van Asch CJ, Luitse MJ, Rinkel GJ, et al. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta‐analysis. Lancet Neurol 2010;9:167–176. - PubMed
-
- Gross BA, Jankowitz BT, Friedlander RM. Cerebral Intraparenchymal hemorrhage: a review. JAMA 2019;321:1295–1303. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
