

Metabolic phenotyping by treatment modality in obese women with gestational diabetes suggests diverse pathophysiology: An exploratory study
- PMID: 32240196
- PMCID: PMC7117764
- DOI: 10.1371/journal.pone.0230658
Metabolic phenotyping by treatment modality in obese women with gestational diabetes suggests diverse pathophysiology: An exploratory study
Abstract
Background and purpose: Excess insulin resistance is considered the predominant pathophysiological mechanism in obese women who develop gestational diabetes (GDM). We hypothesised that obese women requiring differing treatment modalities for GDM may have diverse underlying metabolic pathways.
Methods: In this secondary analysis of the UK pregnancies Better Eating and Activity Trial (UPBEAT) we studied women from the control arm with complete biochemical data at three gestational time points; at 15-18+6 and 27-28+6 weeks (before treatment), and 34-36+0 weeks (after treatment). A total of 89 analytes were measured (plasma/serum) using a targeted nuclear magnetic resonance (NMR) platform and conventional assays. We used linear regression with appropriate adjustment to model metabolite concentration, stratified by treatment group.
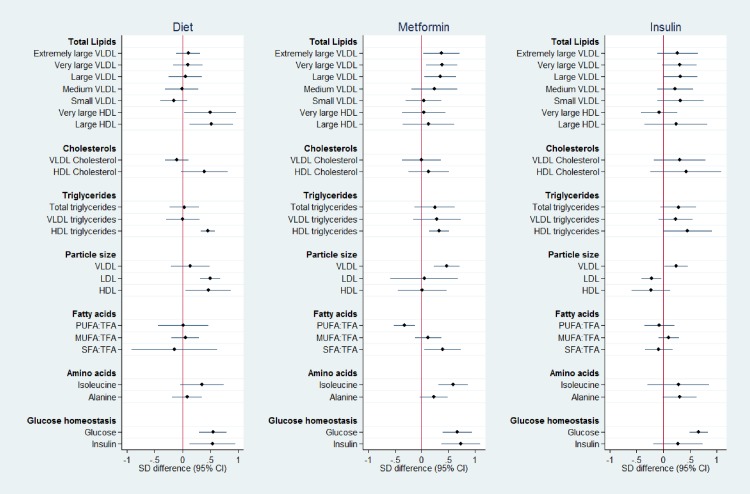
Main findings: 300 women (median BMI 35kg/m2; inter quartile range 32.8-38.2) were studied. 71 developed GDM; 28 received dietary treatment only, 20 metformin, and 23 received insulin. Prior to the initiation of treatment, multiple metabolites differed (p<0.05) between the diet and insulin-treated groups, especially very large density lipoprotein (VLDL) and high density lipoprotein (HDL) subclasses and constituents, with some differences maintained at 34-36 weeks' gestation despite treatment. Gestational lipid profiles of the diet treatment group were indicative of a lower insulin resistance profile, when compared to both insulin-treated women and those without GDM. At 28 weeks' the diet treatment group had lower plasma fasting glucose and insulin than women treated with insulin, yet similar to those without GDM, consistent with a glycaemic mechanism independent of insulin resistance.
Conclusions/interpretation: This exploratory study suggests that GDM pathophysiological processes may differ amongst obese women who require different treatment modalities to achieve glucose control and can be revealed using metabolic profiling.
Conflict of interest statement
SMN and LP disclose receipt of lecture/other fees from Roche Diagnostics, outside the scope of this work. DAL discloses receipt of fees from Roche Diagnostics and Ferring Pharmaceuticals for research unrelated to this paper. All other authors declare that there is no declaration of interest associated with their contribution to this manuscript. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
