

Labour admission assessment results of index pregnancy as predictors of intrapartum stillbirth in public health facilities of Addis Ababa: A case-control study
- PMID: 32240197
- PMCID: PMC7117700
- DOI: 10.1371/journal.pone.0230478
Labour admission assessment results of index pregnancy as predictors of intrapartum stillbirth in public health facilities of Addis Ababa: A case-control study
Abstract
Background: Approximately one-third of the global stillbirth burden occurs during intrapartum period. The ability to assess obstetric parameters including effacement, dilatation, uterine contraction, decent, rupture of the uterus, and moulding of the foetal head are among the essential competencies required by obstetric service providers admitting women for labour in health facilities. Misdiagnosis of these conditions could result in unnecessary obstetric interventions and unfavourable obstetric outcomes including intrapartum stillbirth. This study aimed to assess associations between missed diagnosis plus complication of labour on admission and intrapartum stillbirth.
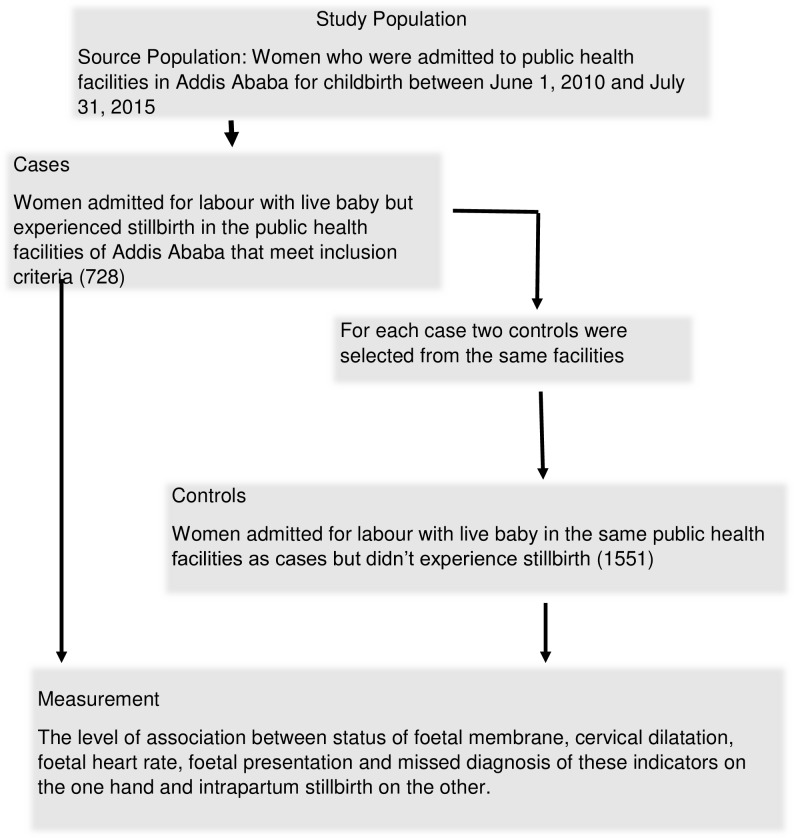
Methods: A case-control study using primary data from chart review of medical records of women who experienced intrapartum stillbirth in 20 public health centres and three public hospitals of Addis Ababa between 01 July 2010 and 30 June 2015 was conducted. Data were collected from charts of all cases meeting the inclusion criteria. Medical records of women with livebirths were randomly selected and reviewed from each public health facilities in two to one (2:1) control to case ratio. Accordingly, 728 cases of stillbirth out of 1,056 charts met the inclusion criteria whereas 1,551 controls out of 1,705 were also considered in the study.
Results: Proportionally, more women in the stillbirth group (39.4%) than in the livebirth group (30.2%) experienced ruptured membrane on admission, with the difference being statistically significant (OR 1.7, 95% CI 1.37-2.03). Significantly higher proportion of women in the intrapartum stillbirth group experienced FRH lower than 110/min, a result suggestive of foetal distress on admission. Proportionally, more women in the intrapartum stillbirth group (14.5%) than in the livebirth group (4.5%) had breech foetal presentation on admission for labour, the difference being statistically significant (aOR 3.26 95% CI 1.93-5.50). Intrapartum stillbirth was slightly higher among women with cervical dilatation 4cm or more on admission (OR 1.2, 95% CI 1.00-1.45). This could be owing to delay in seeking obstetric care or misdiagnosis of the condition, a situation that seeks more rigorous study to determine the underlying causal links. Diagnosis of foetal member was missed among more cases than controls where the difference was statistically significant (aOR 1.51, CI 1.03-2.19).
Conclusion: Low FHR, non-vertex foetal presentations and ruptured cervical membrane were predictors of intrapartum stillbirth. Health facilities could avert unnecessary foetal loss by undertaking timely actions to manage obstetric emergencies on admission to labour.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Consistency and timeliness of intrapartum care interventions as predictors of intrapartum stillbirth in public health facilities of Addis Ababa, Ethiopia: a case-control study.Pan Afr Med J. 2021 Sep 14;40:36. doi: 10.11604/pamj.2021.40.36.25838. eCollection 2021. Pan Afr Med J. 2021. PMID: 34795817 Free PMC article.
-
Maternal and foetal medical conditions during pregnancy as determinants of intrapartum stillbirth in public health facilities of Addis Ababa: a case-control study.Pan Afr Med J. 2019 May 14;33:21. doi: 10.11604/pamj.2019.33.21.17728. eCollection 2019. Pan Afr Med J. 2019. PMID: 31312337 Free PMC article.
-
Inadequate fetal heart rate monitoring and poor use of partogram associated with intrapartum stillbirth: a case-referent study in Nepal.BMC Pregnancy Childbirth. 2016 Aug 19;16:233. doi: 10.1186/s12884-016-1034-5. BMC Pregnancy Childbirth. 2016. PMID: 27542350 Free PMC article.
-
Reducing stillbirths: screening and monitoring during pregnancy and labour.BMC Pregnancy Childbirth. 2009 May 7;9 Suppl 1(Suppl 1):S5. doi: 10.1186/1471-2393-9-S1-S5. BMC Pregnancy Childbirth. 2009. PMID: 19426468 Free PMC article. Review.
-
The intrapartum and perinatal risks of sleep-disordered breathing in pregnancy: a systematic review and metaanalysis.Am J Obstet Gynecol. 2018 Aug;219(2):147-161.e1. doi: 10.1016/j.ajog.2018.02.004. Epub 2018 Feb 15. Am J Obstet Gynecol. 2018. PMID: 29454869
References
-
- Bhutta ZA, Das JK, Bahl R, Lawn JE, Salam RA, Paul VK, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? The Lancet. 2014;384(9940):347–70. - PubMed
-
- Lawn JE, Blencowe H, Pattinson R, Cousens S, Kumar R, Ibiebele I, et al. Stillbirths: Where? When? Why? How to make the data count? The Lancet. 2011;377(9775):1448–63. - PubMed
-
- Marshall J, Raynor M, editors. Myles Textbook for Midwives. Sixth ed London: ELSEVIER; 2014.
-
- WHO. THE P ARTOGRAPH: THE APPLICATION OF THE WHO PARTOGRAPH IN THE MANAGEMENT OF LABOUR. Geneva; 1994.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
