

Yoga-Based Cardiac Rehabilitation After Acute Myocardial Infarction: A Randomized Trial
- PMID: 32241371
- PMCID: PMC7132532
- DOI: 10.1016/j.jacc.2020.01.050
Yoga-Based Cardiac Rehabilitation After Acute Myocardial Infarction: A Randomized Trial
Abstract
Background: Given the shortage of cardiac rehabilitation (CR) programs in India and poor uptake worldwide, there is an urgent need to find alternative models of CR that are inexpensive and may offer choice to subgroups with poor uptake (e.g., women and elderly).
Objectives: This study sought to evaluate the effects of yoga-based CR (Yoga-CaRe) on major cardiovascular events and self-rated health in a multicenter randomized controlled trial.
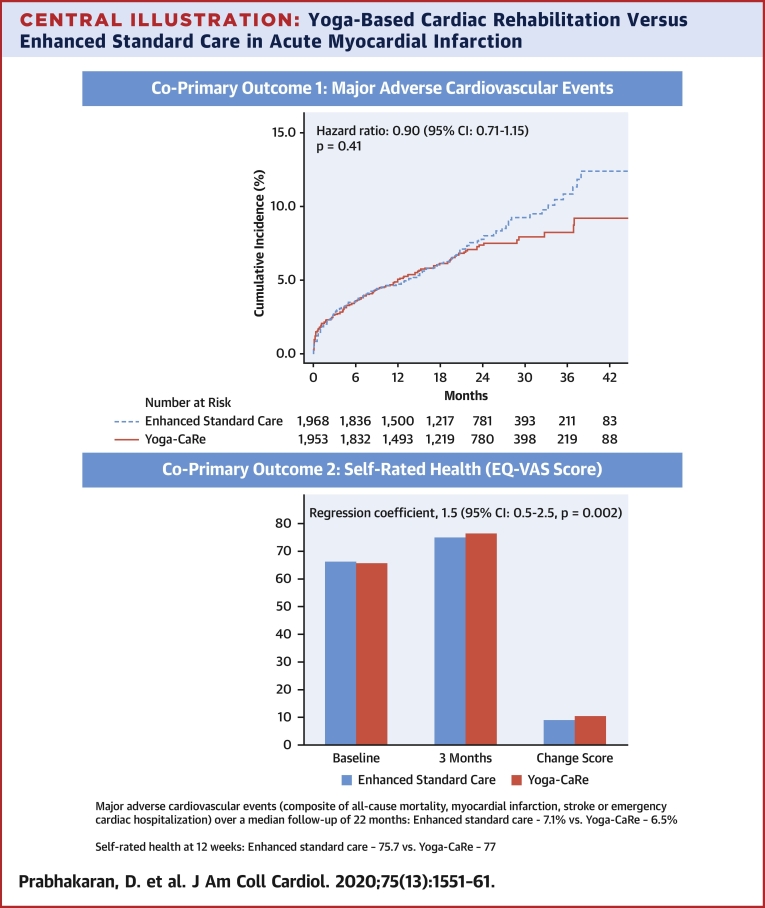
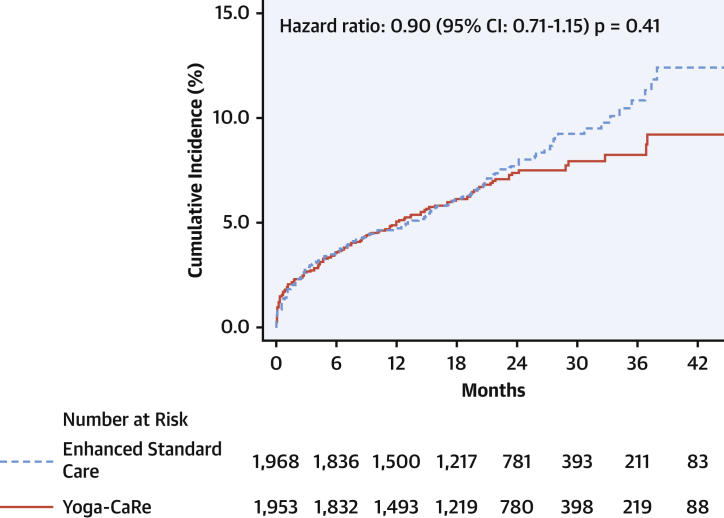
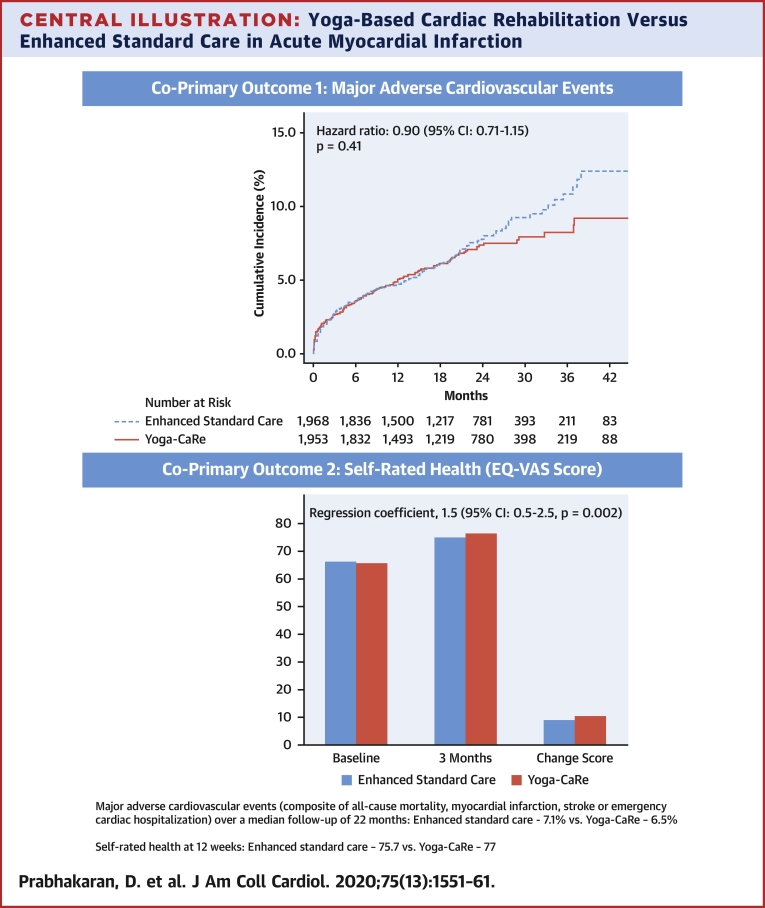
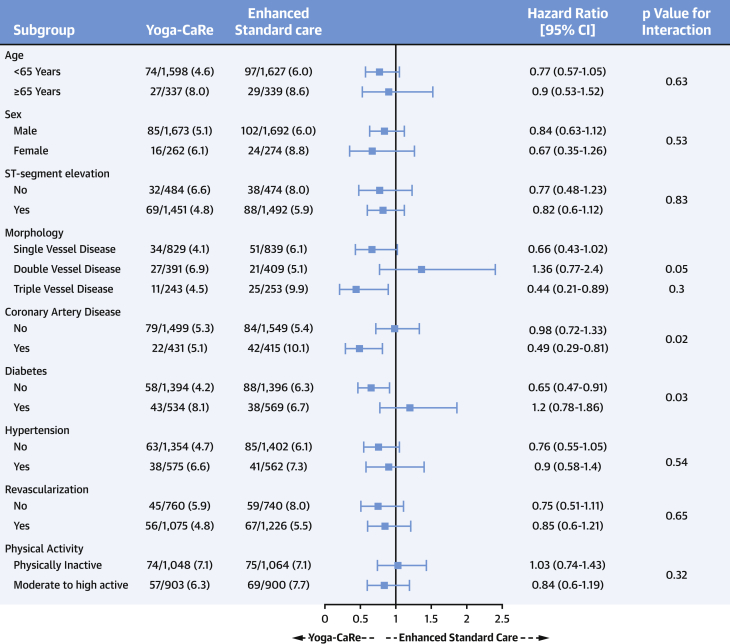
Methods: The trial was conducted in 24 medical centers across India. This study recruited 3,959 patients with acute myocardial infarction with a median and minimum follow-up of 22 and 6 months. Patients were individually randomized to receive either a Yoga-CaRe program (n = 1,970) or enhanced standard care involving educational advice (n = 1,989). The co-primary outcomes were: 1) first occurrence of major adverse cardiovascular events (MACE) (composite of all-cause mortality, myocardial infarction, stroke, or emergency cardiovascular hospitalization); and 2) self-rated health on the European Quality of Life-5 Dimensions-5 Level visual analogue scale at 12 weeks.
Results: MACE occurred in 131 (6.7%) patients in the Yoga-CaRe group and 146 (7.4%) patients in the enhanced standard care group (hazard ratio with Yoga-CaRe: 0.90; 95% confidence interval [CI]: 0.71 to 1.15; p = 0.41). Self-rated health was 77 in Yoga-CaRe and 75.7 in the enhanced standard care group (baseline-adjusted mean difference in favor of Yoga-CaRe: 1.5; 95% CI: 0.5 to 2.5; p = 0.002). The Yoga-CaRe group had greater return to pre-infarct activities, but there was no difference in tobacco cessation or medication adherence between the treatment groups (secondary outcomes).
Conclusions: Yoga-CaRe improved self-rated health and return to pre-infarct activities after acute myocardial infarction, but the trial lacked statistical power to show a difference in MACE. Yoga-CaRe may be an option when conventional CR is unavailable or unacceptable to individuals. (A study on effectiveness of YOGA based cardiac rehabilitation programme in India and United Kingdom; CTRI/2012/02/002408).
Keywords: acute myocardial infarction; cardiac rehabilitation; coronary artery disease; rehabilitation; secondary prevention; yoga.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Expanding Traditional Cardiac Rehabilitation in the 21st Century.J Am Coll Cardiol. 2020 Apr 7;75(13):1562-1564. doi: 10.1016/j.jacc.2020.02.038. J Am Coll Cardiol. 2020. PMID: 32241372 No abstract available.
References
-
- Ibanez B., James S., Agewall S. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39:119–177. - PubMed
-
- Thomas R.J., Balady G., Banka G. 2018 ACC/AHA Clinical performance and quality measures for cardiac rehabilitation: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J Am Coll Cardiol. 2018;71:1814–1837. - PubMed
-
- Ruano-Ravina A., Pena-Gil C., Abu-Assi E. Participation and adherence to cardiac rehabilitation programs. A systematic review. Int J Cardiol. 2016;223:436–443. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
