

Trends in U.S. Burden of Clostridioides difficile Infection and Outcomes
- PMID: 32242357
- PMCID: PMC7861882
- DOI: 10.1056/NEJMoa1910215
Trends in U.S. Burden of Clostridioides difficile Infection and Outcomes
Abstract
Background: Efforts to prevent Clostridioides difficile infection continue to expand across the health care spectrum in the United States. Whether these efforts are reducing the national burden of C. difficile infection is unclear.
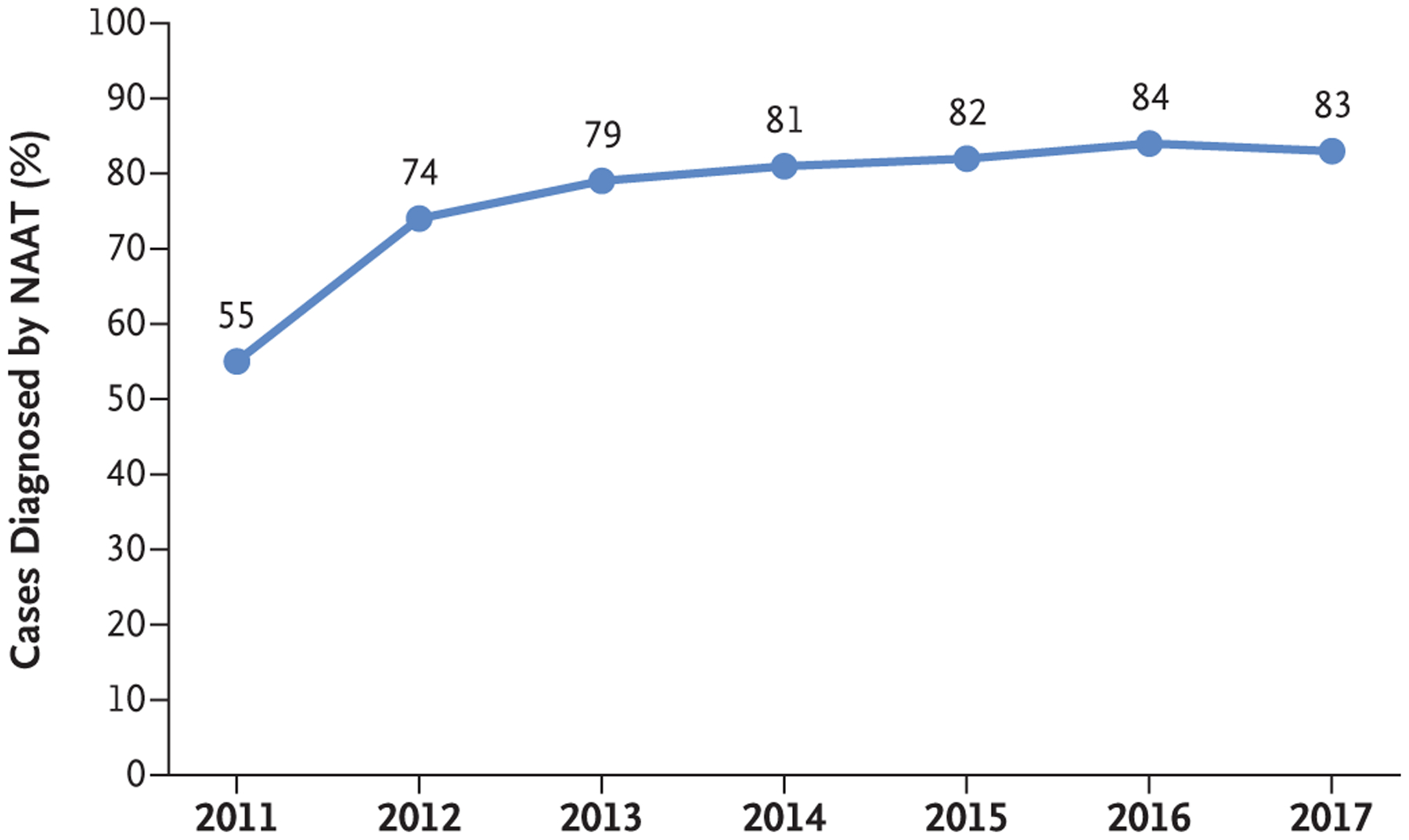
Methods: The Emerging Infections Program identified cases of C. difficile infection (stool specimens positive for C. difficile in a person ≥1 year of age with no positive test in the previous 8 weeks) in 10 U.S. sites. We used case and census sampling weights to estimate the national burden of C. difficile infection, first recurrences, hospitalizations, and in-hospital deaths from 2011 through 2017. Health care-associated infections were defined as those with onset in a health care facility or associated with recent admission to a health care facility; all others were classified as community-associated infections. For trend analyses, we used weighted random-intercept models with negative binomial distribution and logistic-regression models to adjust for the higher sensitivity of nucleic acid amplification tests (NAATs) as compared with other test types.
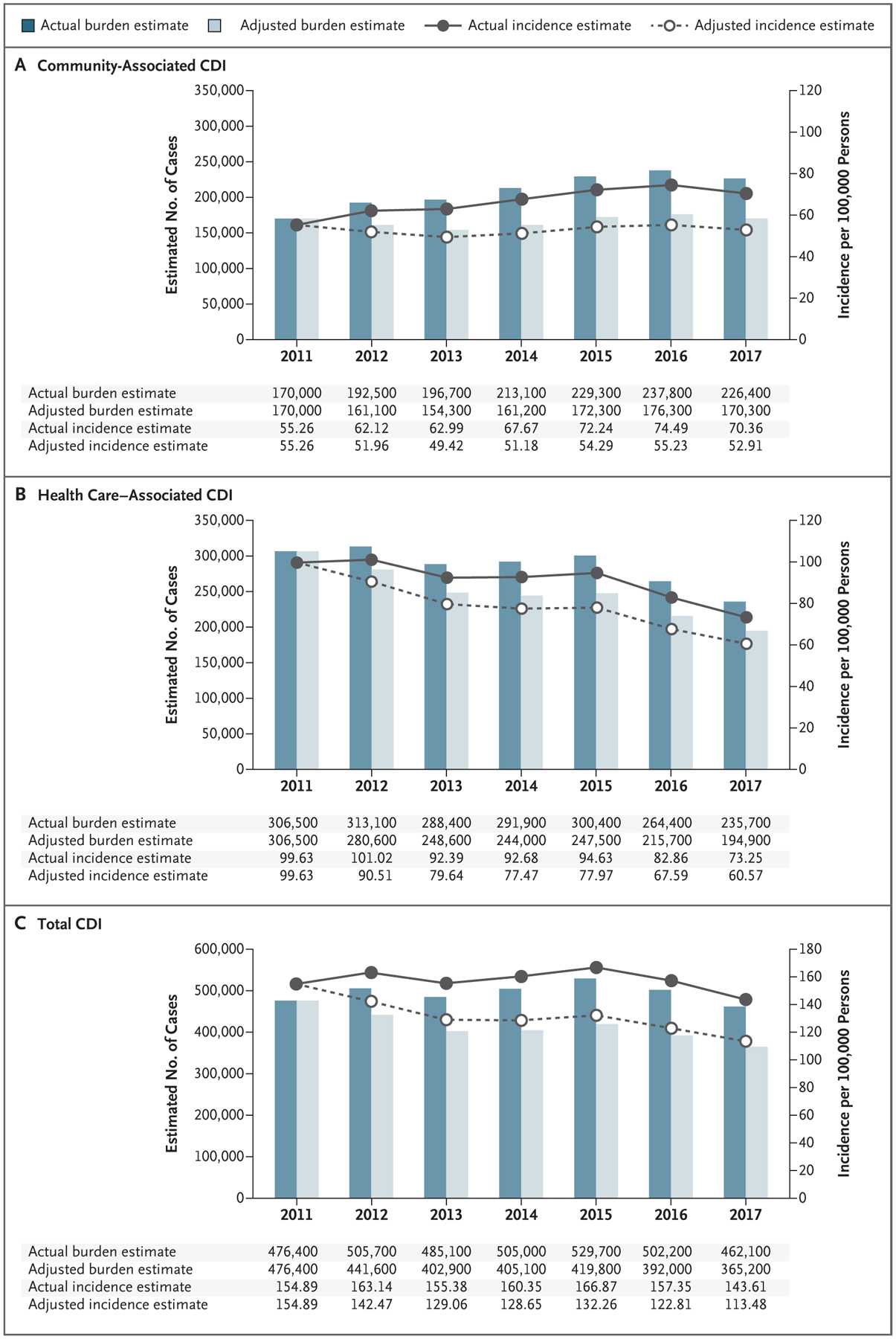
Results: The number of cases of C. difficile infection in the 10 U.S. sites was 15,461 in 2011 (10,177 health care-associated and 5284 community-associated cases) and 15,512 in 2017 (7973 health care-associated and 7539 community-associated cases). The estimated national burden of C. difficile infection was 476,400 cases (95% confidence interval [CI], 419,900 to 532,900) in 2011 and 462,100 cases (95% CI, 428,600 to 495,600) in 2017. With accounting for NAAT use, the adjusted estimate of the total burden of C. difficile infection decreased by 24% (95% CI, 6 to 36) from 2011 through 2017; the adjusted estimate of the national burden of health care-associated C. difficile infection decreased by 36% (95% CI, 24 to 54), whereas the adjusted estimate of the national burden of community-associated C. difficile infection was unchanged. The adjusted estimate of the burden of hospitalizations for C. difficile infection decreased by 24% (95% CI, 0 to 48), whereas the adjusted estimates of the burden of first recurrences and in-hospital deaths did not change significantly.
Conclusions: The estimated national burden of C. difficile infection and associated hospitalizations decreased from 2011 through 2017, owing to a decline in health care-associated infections. (Funded by the Centers for Disease Control and Prevention.).
Copyright © 2020 Massachusetts Medical Society.
Figures
References
-
- Elixhauser A, Jhung MA. Clostridium difficile-associated disease in U.S. hospitals, 1993–2005: Healthcare Cost and Utilization Project statistical brief #50. Rockville, MD: Agency for Healthcare research and Quality, April 2008. (http://www.hcup-us.ahrq.gov/reports/statbriefs/sb50.pdf).
-
- Layton BA, McDonald LC, Gerding DN, Liedtke LA, Strausbaugh LJ. Perceived increases in the incidence and severity of Clostridium difficile disease: an emerging threat that continues to unfold. In: Proceedings of 15th Annual Scientific Meeting of the Society for Healthcare Epidemiology of America, Los Angeles, April 9–12, 2005 abstract.
-
- Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile–associated diarrhea with high morbidity and mortality. N Engl J Med 2005; 353: 2442–9. - PubMed
-
- McDonald LC, Killgore GE, Thompson A, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med 2005; 353: 2433–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical