

Association Between Financial Incentives in Medicare's Hospital Readmissions Reduction Program and Hospital Readmission Performance
- PMID: 32242906
- PMCID: PMC7125432
- DOI: 10.1001/jamanetworkopen.2020.2044
Association Between Financial Incentives in Medicare's Hospital Readmissions Reduction Program and Hospital Readmission Performance
Abstract
Importance: The strongest evidence for the effectiveness of Medicare's Hospital Readmissions Reduction Program (HRRP) involves greater reductions in readmissions for hospitals receiving penalties compared with those not receiving penalties. However, the HRRP penalty is an imperfect measure of hospitals' marginal incentive to avoid a readmission for HRRP-targeted diagnoses.
Objectives: To assess the association between hospitals' condition-specific incentives and readmission performance and to examine the responsiveness of hospitals to condition-specific incentives compared with aggregate penalty amounts.
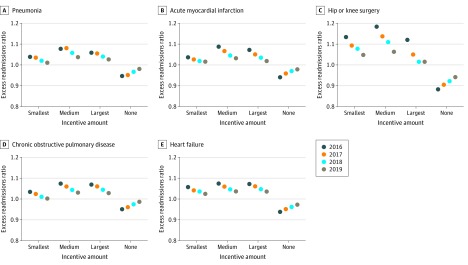
Design, setting, and participants: This retrospective cohort analysis used Medicare readmissions data from 2823 US short-term acute care hospitals participating in HRRP to compare 3-year (fiscal years 2016-2019) follow-up readmission performance according to tertiles of hospitals' baseline (2016) marginal incentives for each of 5 HRRP-targeted conditions (acute myocardial infarction, heart failure, chronic obstructive pulmonary disease, pneumonia, and hip and/or knee surgery).
Main outcomes and measures: Linear regression models were used to estimate mean change in follow-up readmission performance, measured using the excess readmissions ratio, with baseline condition-specific incentives and aggregate penalty amounts.
Results: Of 2823 hospitals that participated in the HRRP from baseline to follow-up, 2280 (81%) had more than 1 excess readmission for 1 or more applicable condition and 543 (19%) did not have any excess readmissions. The mean (SD) financial incentive to reduce readmissions for incentivized hospitals ranged from $8762 ($3699) to $58 158 ($26 198) per 1 avoided readmission. Hospitals with greater incentives for readmission avoidance had greater decreases in readmissions compared with hospitals with smaller incentives (45% greater for pneumonia, 172% greater for acute myocardial infarction, 40% greater for hip and/or knee surgery, 32% greater for chronic obstructive pulmonary disease, and 13% greater for heart failure), whereas hospitals with no incentives had increases in excess readmissions of 4% to 7% (median, 4% [percentage change for nonincentivized hospitals was 3.7% for pneumonia, 4.2% for acute myocardial infarction, 7.1% for hip and/or knee surgery, 3.7% for chronic obstructive pulmonary disease, and 3.7% for heart failure]; P < .001). During the study period, each additional $5000 in the incentive amount was associated with a 0.6- to 1.3-percentage point decrease, or up to a 26% decrease, in excess readmissions (P < .001). Regression to the mean explained approximately one-third of the results depending on the condition examined.
Conclusions and relevance: The findings suggest that improvements in readmission avoidance are more strongly associated with incentives from the HRRP than with aggregate penalty amounts, suggesting that the program has elicited sizeable changes. Worsened performance among hospitals with small or no incentives may indicate the need for reconsideration of the program's lack of financial rewards for high-performing hospitals.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
