

Risk Estimates Supporting the 2019 ASCCP Risk-Based Management Consensus Guidelines
- PMID: 32243308
- PMCID: PMC7147417
- DOI: 10.1097/LGT.0000000000000529
Risk Estimates Supporting the 2019 ASCCP Risk-Based Management Consensus Guidelines
Abstract
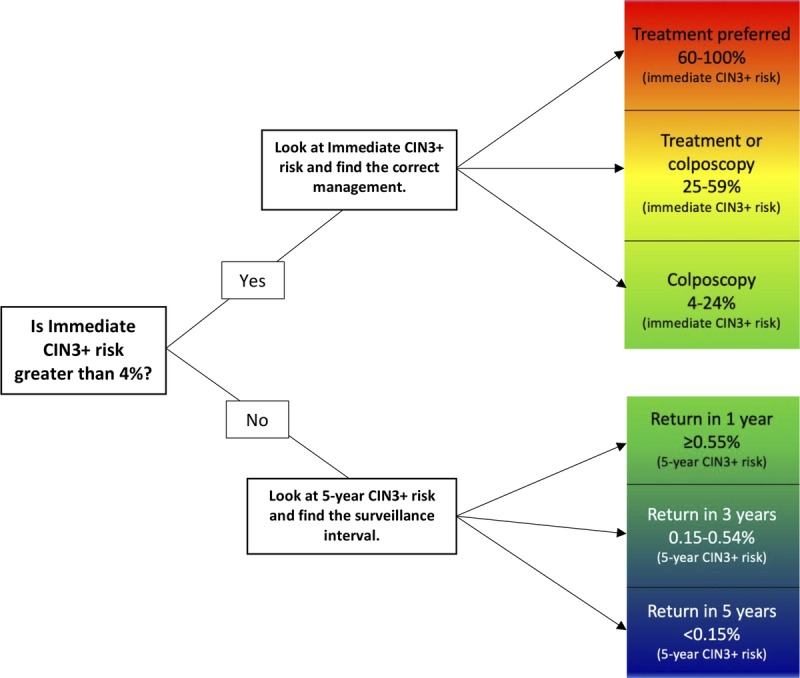
The 2019 American Society for Colposcopy and Cervical Pathology Risk-Based Management Consensus Guidelines for the management of cervical cancer screening abnormalities recommend 1 of 6 clinical actions (treatment, optional treatment or colposcopy/biopsy, colposcopy/biopsy, 1-year surveillance, 3-year surveillance, 5-year return to regular screening) based on the risk of cervical intraepithelial neoplasia grade 3, adenocarcinoma in situ, or cancer (CIN 3+) for the many different combinations of current and recent past screening results. This article supports the main guidelines presentation by presenting and explaining the risk estimates that supported the guidelines.
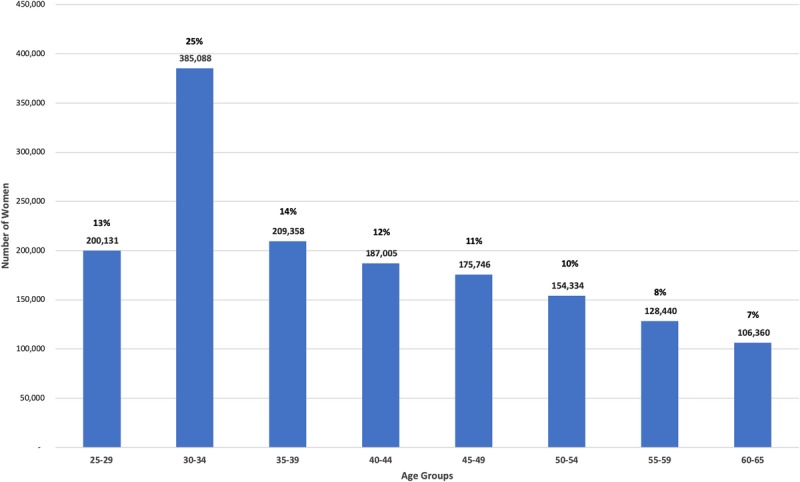
Methods: From 2003 to 2017 at Kaiser Permanente Northern California (KPNC), 1.5 million individuals aged 25 to 65 years were screened with human papillomavirus (HPV) and cytology cotesting scheduled every 3 years. We estimated immediate and 5-year risks of CIN 3+ for combinations of current test results paired with history of screening test and colposcopy/biopsy results.
Results: Risk tables are presented for different clinical scenarios. Examples of important results are highlighted; for example, the risk posed by most current abnormalities is greatly reduced if the prior screening round was HPV-negative. The immediate and 5-year risks of CIN 3+ used to decide clinical management are shown.
Conclusions: The new risk-based guidelines present recommendations for the management of abnormal screening test and histology results; the key risk estimates supporting guidelines are presented in this article. Comprehensive risk estimates are freely available online at https://CervixCa.nlm.nih.gov/RiskTables.
Conflict of interest statement
The National Cancer Institute (including M.S. and N.W.) has received cervical screening results at reduced or no cost from commercial research partners (Qiagen, Roche, BD, MobileODT, Arbor Vita) for independent evaluations of screening methods and strategies. P.E.C. has received HPV tests and assays at a reduced or no cost from Roche, Becton Dickinson, Arbor Vita Corporation, and Cepheid for research. R.S.G. reports that he was an ASCCP consultant for the guideline and a DSMB consultant for Ikonosys. The other authors have declared they have no conflicts of interest.
Figures
References
-
- Massad LS, Einstein MH, Huh WK, et al. 2012 updated consensus guidelines for the management of abnormal cervical cancer screening tests and cancer precursors. J Low Genit Tract Dis 2013;17:S1–27. - PubMed
