

Serologic surveillance of maternal Zika infection in a prospective cohort in Leon, Nicaragua during the peak of the Zika epidemic
- PMID: 32243482
- PMCID: PMC7122769
- DOI: 10.1371/journal.pone.0230692
Serologic surveillance of maternal Zika infection in a prospective cohort in Leon, Nicaragua during the peak of the Zika epidemic
Abstract
Background: Zika virus caused thousands of congenital anomalies during a recent epidemic. Because Zika emerged in areas endemic for dengue and these related flaviviruses elicit cross-reactive antibodies, it is challenging to serologically monitor pregnant women for Zika infection.
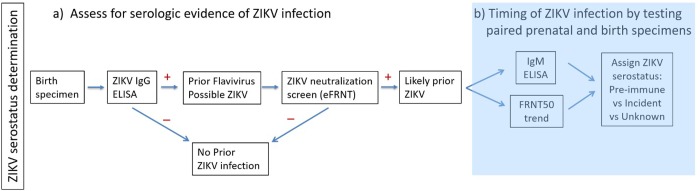
Methods: A prospective cohort of 253 pregnant women was established in León, Nicaragua. Women were followed during prenatal care through delivery. Serologic specimens were obtained at each visit, and birth outcome was recorded. Established flavivirus serologic methods were adapted to determine Zika seroprevalence, and a stepwise testing algorithm estimated timing of Zika infection in relation to pregnancy.
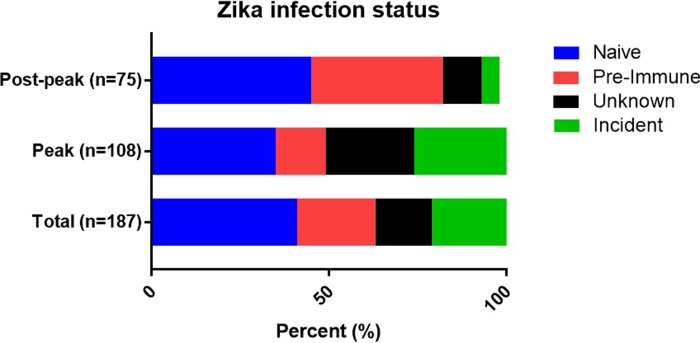
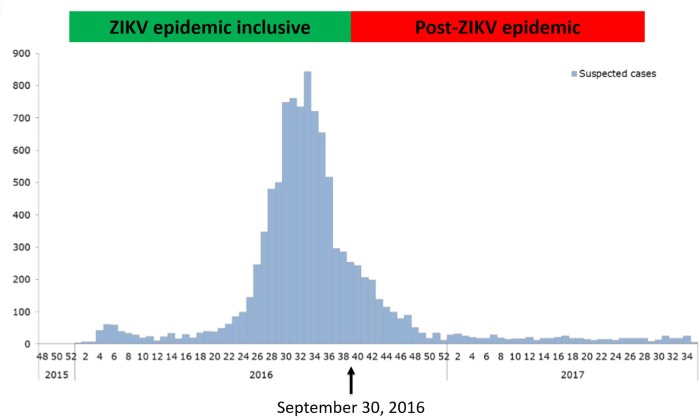
Results: Zika seroprevalence was approximately 59% among women tested. Neutralization testing was highly concordant with Zika NS1 BOB results. Per study algorithm, 21% (40/187) of women were classified as experiencing Incident ZIKV infection during pregnancy. Importantly, the Incident ZIKV group included mostly women pregnant during the 2016 Zika epidemic peak and the only 3 subjects in the cohort with RT-PCR-confirmed infections. Approximately 17% of births had complications; 1.5% (3/194) manifesting clinical criteria of congenital Zika syndrome, one was RT-PCR-confirmed as a case of congenital Zika syndrome. Adverse birth outcome did not correlate with timing of Zika infection.
Conclusions: By leveraging prenatal care systems, we developed a simple algorithm for identifying women who were likely infected by Zika during pregnancy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- França GVA, Schuler-Faccini L, Oliveira WK, Henriques CMP, Carmo EH, Pedi VD, et al. Congenital Zika virus syndrome in Brazil: a case series of the first 1501 livebirths with complete investigation. Lancet (London, England). 2016. August 27;388(10047):891–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
