

Left atrial appendage occlusion with the Amplatzer™ Amulet™ device: full results of the prospective global observational study
- PMID: 32243499
- PMCID: PMC7421773
- DOI: 10.1093/eurheartj/ehaa169
Left atrial appendage occlusion with the Amplatzer™ Amulet™ device: full results of the prospective global observational study
Abstract
Aims: To evaluate the safety and efficacy of left atrial appendage occlusion (LAAO) with the Amplatzer™ Amulet™ occluder.
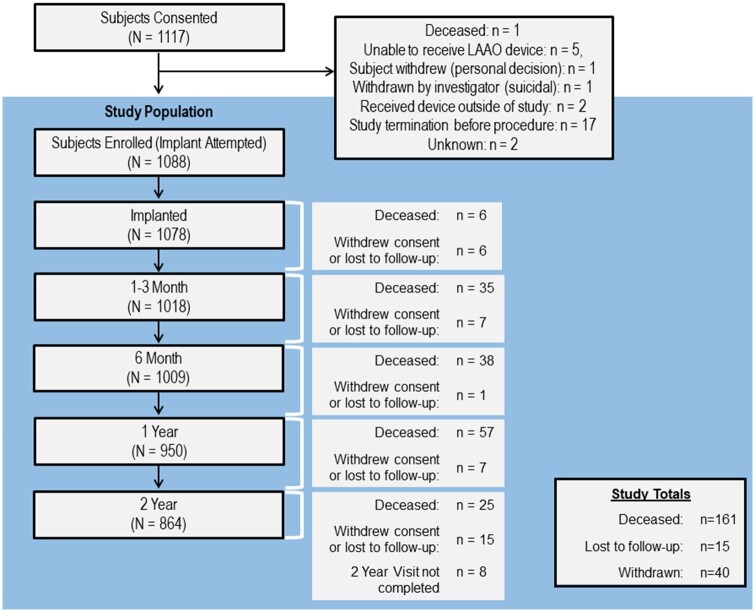
Methods and results: Patients with atrial fibrillation eligible for LAAO were recruited to a prospective global study. Implant procedures were undertaken with echocardiographic guidance. Transoesophageal echocardiography (TOE) was undertaken 1-3 months post-LAAO. Implant and follow-up TOEs were evaluated by a CoreLab. The primary endpoint was a composite of ischaemic stroke and cardiovascular death at 2 years. Serious adverse events were adjudicated by an independent clinical events committee. A total of 1088 patients were enrolled, aged 75.2 ± 8.5 years; 64.5% were male. CHA2DS2-VASc and HAS-BLED scores were 4.2 ± 1.6 and 3.3 ± 1.1, respectively. A total of 71.7% had prior major bleeding, and 82.8% had contraindications to oral anticoagulants. Implant success was 99.1%. Major adverse events (≤7 days post-procedure) occurred in 4.0%, including death (0.3%), stroke (0.4%), major vascular (1.3%), and device embolization (0.2%). A total of 80.2% of patients were discharged on antiplatelet therapy alone. Peridevice flow was <3 mm in 98.4% at follow-up TOE. Device-related thrombus (DRT) was seen in 1.6% of cases. Cardiovascular death or ischaemic stroke occurred in 8.7% of patients at 2 years. The ischaemic stroke rate was 2.2%/year-a 67% reduction compared to the CHA2DS2-VASc predicted rate. Major bleeding (Bleeding Academic Research Consortium type ≥ 3) occurred at rates of 10.1%/year (year 1) and 4.0%/year (year 2).
Conclusion: Following LAAO with the Amplatzer Amulet device, the ischaemic stroke rate was reduced by 67% compared to the predicted risk. Closure was complete in 98.4% of cases and DRT seen in only 1.6%.
Keywords: Antithrombotic treatment; Bleeding; Death; LAA closure; Stroke.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures


Comment in
-
Rebellious palpitations.Eur Heart J. 2020 Aug 7;41(30):2902-2903. doi: 10.1093/eurheartj/ehaa261. Eur Heart J. 2020. PMID: 32385490 No abstract available.
-
Association between device-related thrombus and the neo-appendage with left-atrial appendage occlusion devices.Eur Heart J. 2021 Mar 7;42(10):1047-1048. doi: 10.1093/eurheartj/ehaa803. Eur Heart J. 2021. PMID: 33167004 No abstract available.
-
Left atrial appendage occlusion and device-related thrombus: keeping a lid on it.Eur Heart J. 2021 Mar 7;42(10):1049. doi: 10.1093/eurheartj/ehaa806. Eur Heart J. 2021. PMID: 33167037 No abstract available.
References
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener H-C, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P; ESC Scientific Document Group. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37:2893–2962. - PubMed
-
- Ball J, Carrington MJ, McMurray JJ, Stewart S. Atrial fibrillation: profile and burden of an evolving epidemic in the 21st century. Int J Cardiol 2013;167:1807–1824. - PubMed
-
- Lin H-J, Wolf PA, Kelly-Hayes M, Beiser AS, Kase CS, Benjamin EJ, D'Agostino RB. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996;27:1760–1764. - PubMed
-
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr, Ellinor PT, Ezekowitz MD, Field ME, Furie KL, Heidenreich PA, Murray KT, Shea JB, Tracy CM, Yancy CW. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2019;74:104–132. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
