

Subclinical imaging changes in cerebral cavernous angiomas during prospective surveillance
- PMID: 32244216
- PMCID: PMC7541547
- DOI: 10.3171/2020.1.JNS193479
Subclinical imaging changes in cerebral cavernous angiomas during prospective surveillance
Abstract
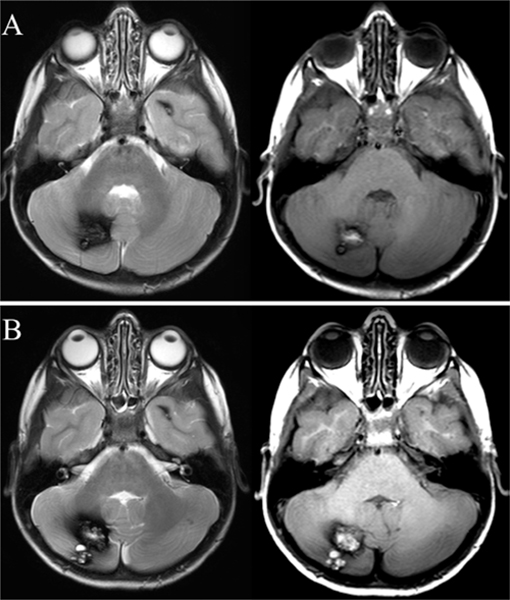
Objective: The purpose of this study was to systematically assess asymptomatic changes (ACs), including subclinical hemorrhage, growth, or new lesion formation (NLF) during longitudinal follow-up of cerebral cavernous angiomas (CAs), and to correlate these with symptomatic hemorrhage (SH) during the same period and with clinical features of the disease.
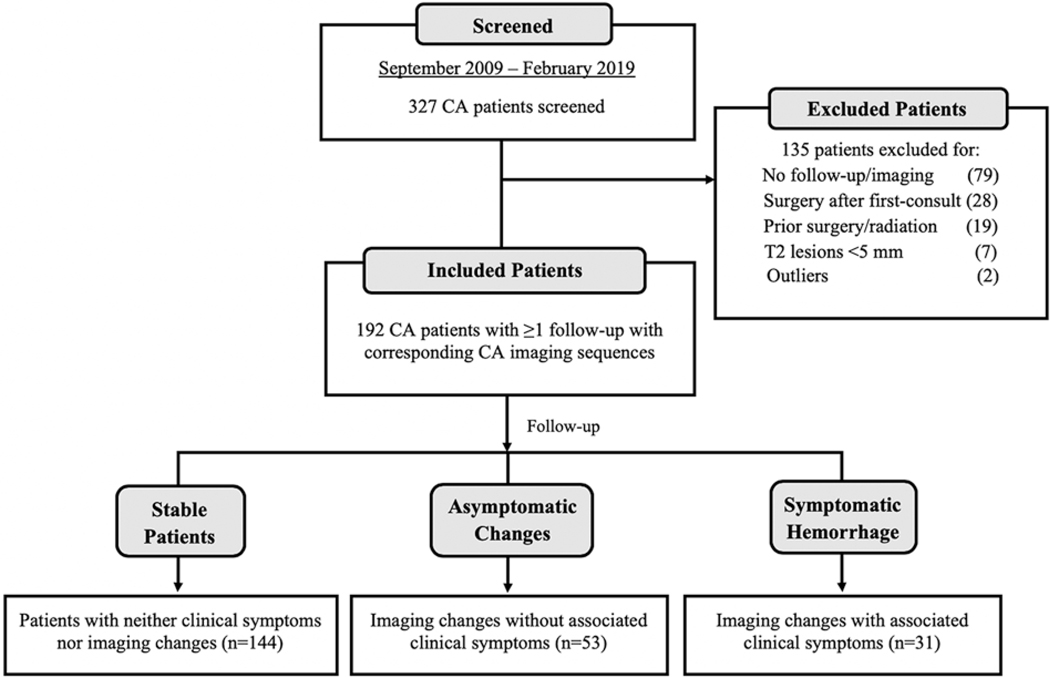
Methods: One hundred ninety-two patients were included in this study, among 327 consecutive patients with CA, prospectively identified between September 2009 and February 2019. Included patients had undergone clinical and MRI follow-up, in conjunction with institutional review board-approved biomarker studies, and harbored ≥ 1 CA with a maximum diameter of ≥ 5 mm on T2-weighted MRI. Rates of AC and SH per lesion-year and patient-year were assessed using prospectively articulated criteria. In multifocal/familial cases, rates of NLF were also assessed.
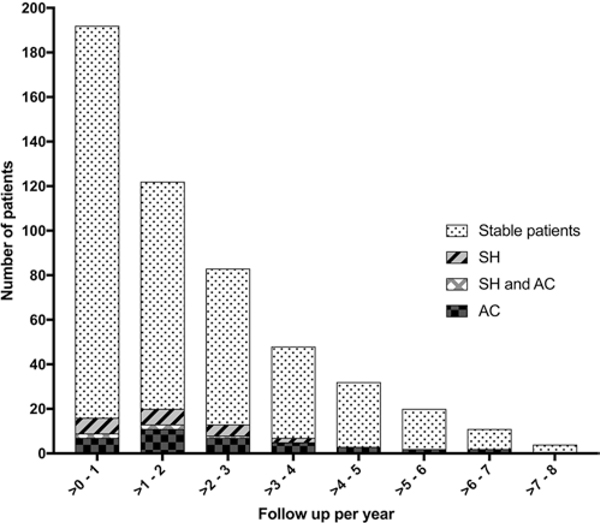
Results: There were no differences in demographic or disease features among cases included or excluded in the study cohort, except for a higher proportion of included patients with CCM3 mutation. Follow-up was 411 patient-years (2503 lesion-years). The rate of AC was higher than the rate of SH (12.9% vs 7.5% per patient-year, and 2.1% vs 1.2% per lesion-year, both p = 0.02). Patients presenting with a prior history of SH had a higher rate of AC than those with other forms of presentation (19.7% and 8.2% per patient-year, respectively; p = 0.003). A higher rate of NLF on T2-weighted MRI (p = 0.03) was observed in patients with prior SH. Three of 6 solitary/sporadic and 2 of 28 multifocal/familial patients underwent resection of the lesion after AC.
Conclusions: Rates of AC are greater than SH during prospective follow-up of CAs, and greater in cases with prior SH. AC may be a more sensitive biomarker of lesional activity, and a more efficient surrogate outcome in clinical trials than SH. Patients experiencing an AC are more likely to undergo a surgical intervention when CAs are solitary/sporadic than when they are multifocal/familial.
Keywords: cerebral cavernous hemangioma; cerebrovascular disorders; intracranial hemorrhage; magnetic resonance imaging; natural history; vascular disorders.
Figures
References
-
- Akers A, Al-Shahi Salman R, Awad IA, et al. Synopsis of Guidelines for the Clinical Management of Cerebral Cavernous Malformations: Consensus Recommendations Based on Systematic Literature Review by the Angioma Alliance Scientific Advisory Board Clinical Experts Panel. Neurosurgery. 2017;80(5):665–680. - PMC - PubMed
-
- Al-Holou WN, O’Lynnger TM, Pandey AS, et al. Natural history and imaging prevalence of cavernous malformations in children and young adults. J Neurosurg Pediatr. 2012;9(2):198–205. - PubMed
-
- Robinson JR Jr, Awad IA, Masaryk TJ, Estes ML. Pathological heterogeneity of angiographically occult vascular malformations of the brain. Neurosurgery. 1993;33(4):547–555. - PubMed
-
- Shimizu Y, Sasaki K, Ujiie H, et al. Pathological findings of angiographically occult vascular malformation. J Clin Neurosci. 2002;9(suppl 1):19–21. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
