

Maintaining Preparedness to Severe Though Infrequent Threats-Can It Be Done?
- PMID: 32244530
- PMCID: PMC7177483
- DOI: 10.3390/ijerph17072385
Maintaining Preparedness to Severe Though Infrequent Threats-Can It Be Done?
Abstract
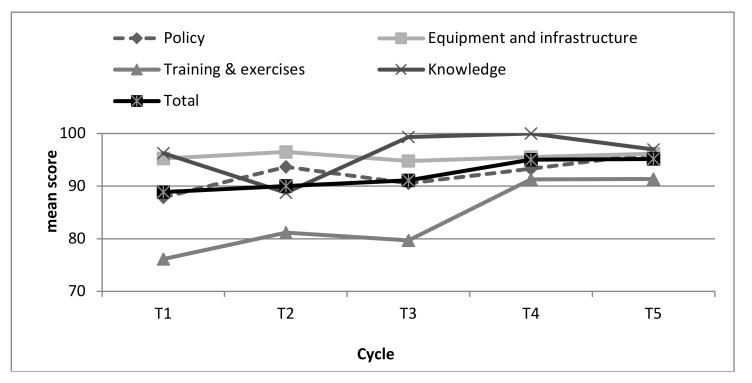
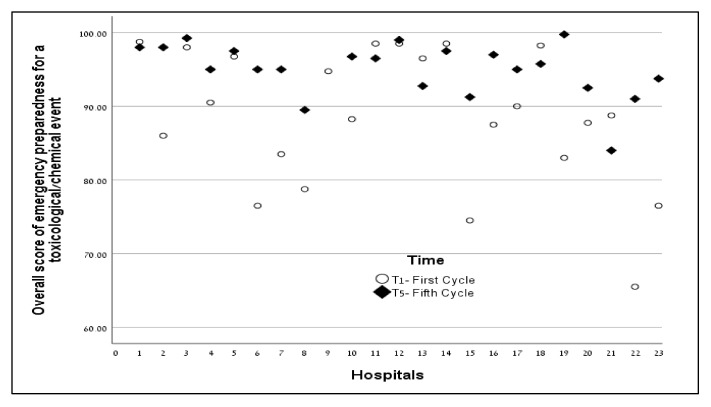
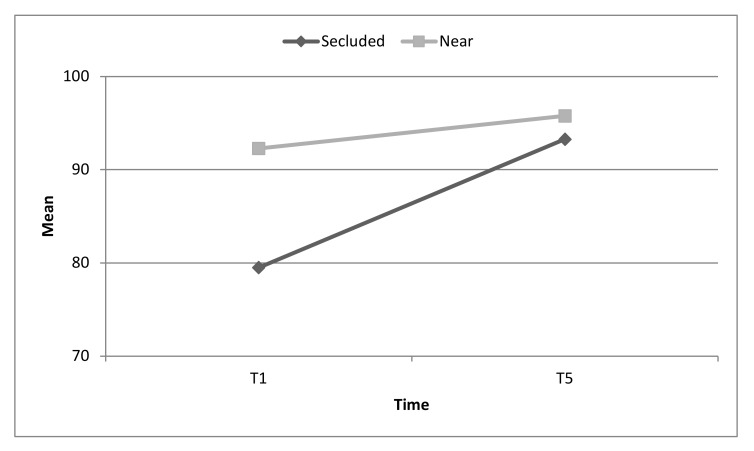
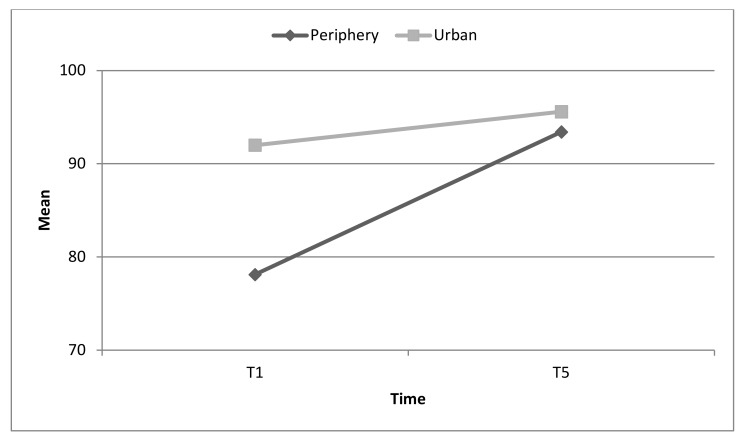
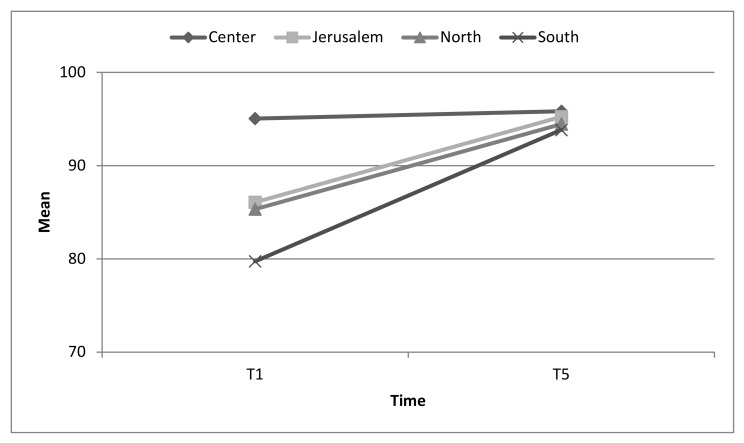
Background: A mass casualty incident (MCI) caused by toxicological/chemical materials constitutes a potential though uncommon risk that may cause great devastation. Presentation of casualties exposed to such materials in hospitals, if not immediately identified, may cause secondary contamination resulting in dysfunction of the emergency department. The study examined the impact of a longitudinal evaluation process on the ongoing emergency preparedness of hospitals for toxicological MCIs, over a decade. Methods: Emergency preparedness for toxicological incidents of all Israeli hospitals were periodically evaluated, over ten years. The evaluation was based on a structured tool developed to encourage ongoing preparedness of Standard Operating Procedures (SOPs), equipment and infrastructure, knowledge of personnel, and training and exercises. The benchmarks were distributed to all hospitals, to be used as a foundation to build and improve emergency preparedness. Scores were compared within and between hospitals. Results: Overall mean scores of emergency preparedness increased over the five measurements from 88 to 95. A significant increase between T1 (first evaluation) and T5 (last evaluation) occurred in SOPs (p = 0.006), training and exercises (p = 0.003), and in the overall score (p = 0.004). No significant changes were found concerning equipment and infrastructure and knowledge; their scores were consistently very high throughout the decade. An interaction effect was found between the cycles of evaluation and the hospitals' geographical location (F (1,20) = 3.0, p = 0.056), proximity to other medical facilities (F (1,20) = 10.0 p = 0.005), and type of area (Urban vs. Periphery) (F (1,20) = 13.1, p = 0.002). At T5, all hospitals achieved similar high scores of emergency preparedness. Conclusions: Use of accessible benchmarks, which clearly delineate what needs to be continually implemented, facilitates an ongoing sustenance of effective levels of emergency preparedness. As this was demonstrated for a risk that does not frequently occur, it may be assumed that it is possible and practical to achieve and maintain emergency preparedness for other potential risks.
Keywords: benchmarks; emergency preparedness; evaluation; mass casualty incident; toxicological/chemical event.
Conflict of interest statement
There are no conflicts of interests to any of the authors.
Figures
Similar articles
-
Improving hospital mass casualty preparedness through ongoing readiness evaluation.Am J Med Qual. 2012 Sep-Oct;27(5):426-33. doi: 10.1177/1062860611432303. Epub 2012 Feb 10. Am J Med Qual. 2012. PMID: 22326978
-
Adequacy of US Hospital Security Preparedness for Mass Casualty Incidents: Critical Lessons From the Israeli Experience.J Public Health Manag Pract. 2016 Jan-Feb;22(1):68-80. doi: 10.1097/PHH.0000000000000298. J Public Health Manag Pract. 2016. PMID: 26594937
-
Assessing and Improving Hospital Mass-Casualty Preparedness: A No-Notice Exercise.Prehosp Disaster Med. 2017 Dec;32(6):662-666. doi: 10.1017/S1049023X17006793. Epub 2017 Aug 7. Prehosp Disaster Med. 2017. PMID: 28780916
-
Use of a Nerve Agent Antidote-Dosing Tool for Mass Casualty Incident Emergency Preparedness.Disaster Med Public Health Prep. 2023 Feb 27;17:e337. doi: 10.1017/dmp.2023.5. Disaster Med Public Health Prep. 2023. PMID: 36847261 Review.
-
Hospital Disasters Preparedness for Mass-Casualty Incidents at Emergency Units in Northwest of Ethiopia: A Cross-Sectional Study.Prehosp Disaster Med. 2023 Jun;38(3):360-365. doi: 10.1017/S1049023X23000365. Epub 2023 Mar 29. Prehosp Disaster Med. 2023. PMID: 36987852 Free PMC article. Review.
Cited by
-
Emotional intelligence, cortisol and α-amylase response to highly stressful hyper-realistic surgical simulation of a mass casualty event scenario.Compr Psychoneuroendocrinol. 2021 Feb 3;5:100031. doi: 10.1016/j.cpnec.2021.100031. eCollection 2021 Feb. Compr Psychoneuroendocrinol. 2021. PMID: 35754451 Free PMC article.
-
Chemical, biological and nerve gas attacks: need for education among healthcare personnel and medical students; a Swedish regional cross-sectional web-survey.BMC Med Educ. 2025 Jan 5;25(1):22. doi: 10.1186/s12909-024-06488-7. BMC Med Educ. 2025. PMID: 39757211 Free PMC article.
References
-
- Valerio A., Verzè M., Marchiori F., Rucci I., De Santis L., Aprili I., Antolini L., Sannino A., Canello A., Checchin E., et al. Managing a mass CO poisoning: Critical issues and solutions from the field to the hyperbaric chamber. Disaster Med. Public Health Prep. 2017;11:251–255. doi: 10.1017/dmp.2016.112. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
