

Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease
- PMID: 32244936
- PMCID: PMC7139690
- DOI: 10.3390/ijms21062135
Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease
Abstract
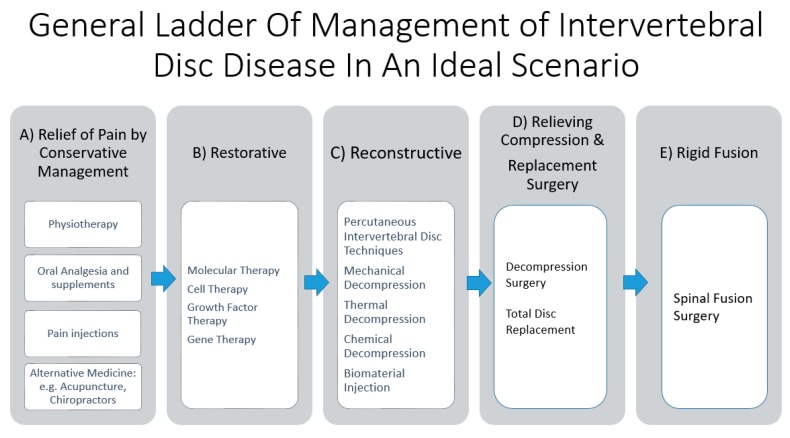
With an aging population, there is a proportional increase in the prevalence of intervertebral disc diseases. Intervertebral disc diseases are the leading cause of lower back pain and disability. With a high prevalence of asymptomatic intervertebral disc diseases, there is a need for accurate diagnosis, which is key to management. A thorough understanding of the pathophysiology and clinical manifestation aids in understanding the natural history of these conditions. Recent developments in radiological and biomarker investigations have potential to provide noninvasive alternatives to the gold standard, invasive discogram. There is a large volume of literature on the management of intervertebral disc diseases, which we categorized into five headings: (a) Relief of pain by conservative management, (b) restorative treatment by molecular therapy, (c) reconstructive treatment by percutaneous intervertebral disc techniques, (d) relieving compression and replacement surgery, and (e) rigid fusion surgery. This review article aims to provide an overview on various current diagnostic and treatment options and discuss the interplay between each arms of these scientific and treatment advancements, hence providing an outlook of their potential future developments and collaborations in the management of intervertebral disc diseases.
Keywords: degenerative disc disease; gene therapy; intervertebral disc; spinal decompression; spinal endoscopy; spinal fusion; spinal injection; spinal molecular therapy; spine pain management; stem cells.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Vos T.P., Flaxman A.D.P., Naghavi M.P., Lozano R.P., Michaud C.M.D., Ezzati M.P., Shibuya K.P., Salomon J.A.P., Abdalla S.M., Aboyans V.P., et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
