

A Novel Predictive Model for In-Hospital Mortality Based on a Combination of Multiple Blood Variables in Patients with ST-Segment-Elevation Myocardial Infarction
- PMID: 32245024
- PMCID: PMC7141500
- DOI: 10.3390/jcm9030852
A Novel Predictive Model for In-Hospital Mortality Based on a Combination of Multiple Blood Variables in Patients with ST-Segment-Elevation Myocardial Infarction
Abstract
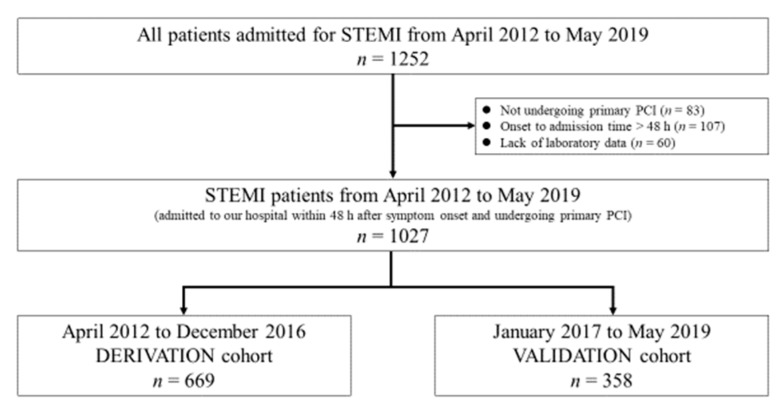
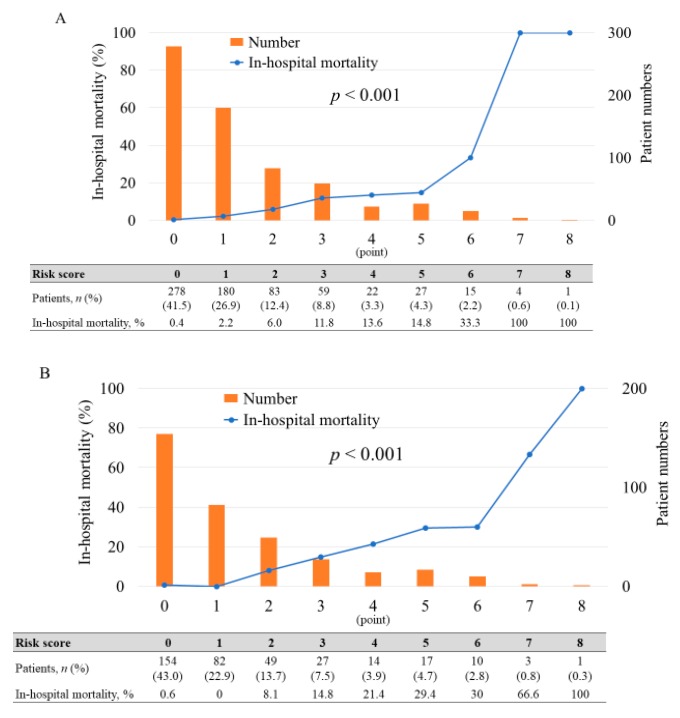
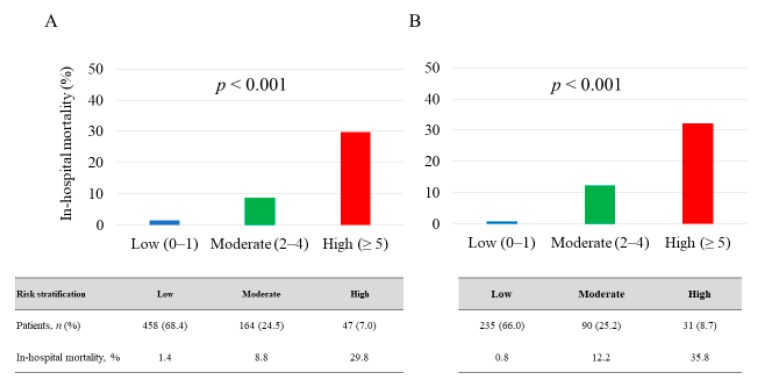
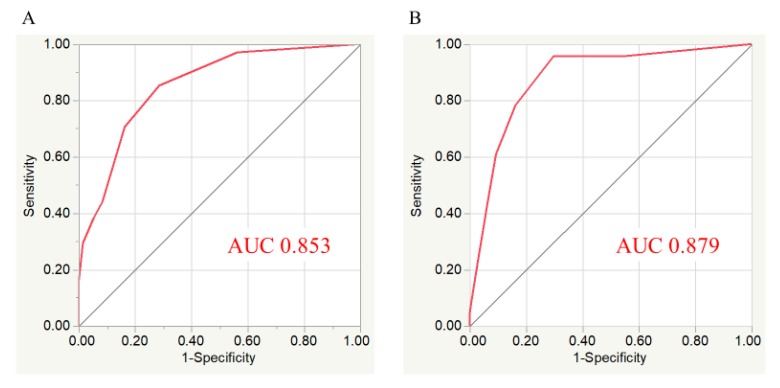
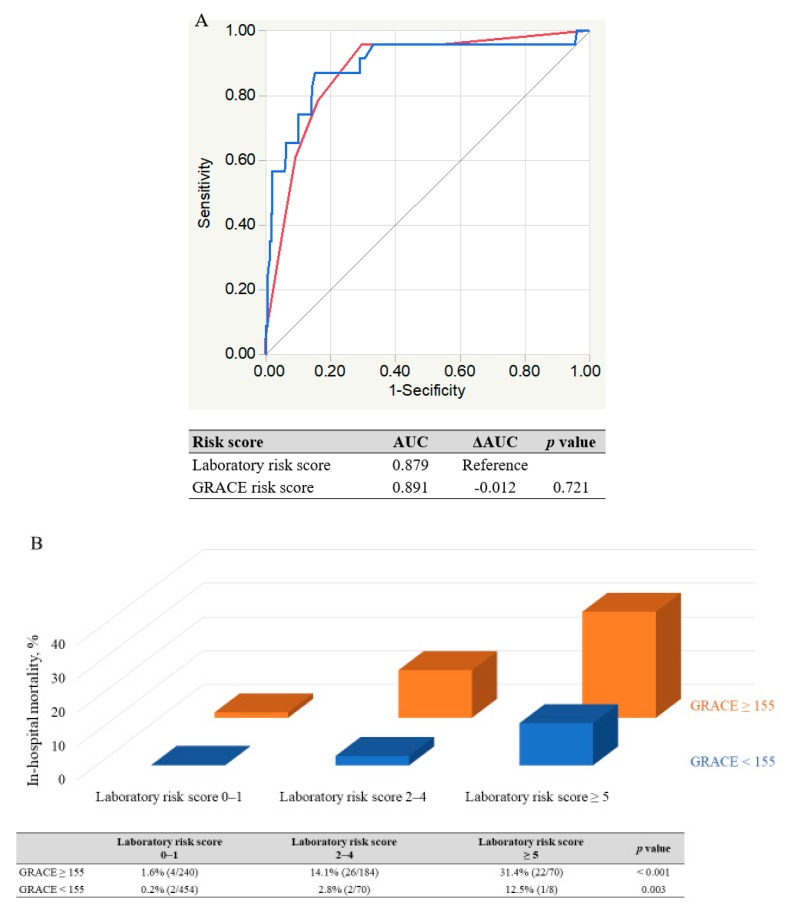
In emergency clinical settings, it may be beneficial to use rapidly measured objective variables for the risk assessment for patient outcome. This study sought to develop an easy-to-measure and objective risk-score prediction model for in-hospital mortality in patients with ST-segment elevation myocardial infarction (STEMI). A total of 1027 consecutive STEMI patients were recruited and divided into derivation (n = 669) and validation (n = 358) cohorts. A risk-score model was created based on the combination of blood test parameters obtained immediately after admission. In the derivation cohort, multivariate analysis showed that the following 5 variables were significantly associated with in-hospital death: estimated glomerular filtration rate <45 mL/min/1.73 m2, platelet count <15 × 104/μL, albumin ≤3.5 g/dL, high-sensitivity troponin I >1.6 ng/mL, and blood sugar ≥200 mg/dL. The risk score was weighted for those variables according to their odds ratios. An incremental change in the scores was significantly associated with elevated in-hospital mortality (p < 0.001). Receiver operating characteristic curve analysis showed adequate discrimination between patients with and without in-hospital death (derivation cohort: area under the curve (AUC) 0.853; validation cohort: AUC 0.879), and there was no significant difference in the AUC values between the laboratory-based and Global Registry of Acute Coronary Events (GRACE) score (p = 0.721). Thus, our laboratory-based model might be helpful in objectively and accurately predicting in-hospital mortality in STEMI patients.
Keywords: ST-segment-elevation myocardial infarction; in-hospital mortality; risk score.
Conflict of interest statement
All authors declare no competing interests.
Figures
References
-
- Ibanez B., James S., Agewall S., Antunes M.J., Bucciarelli-Ducci C., Bueno H., Caforio A.L.P., Crea F., Goudevenos J.A., Halvorsen S., et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur. Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393. - DOI - PubMed
-
- Puymirat E., Simon T., Cayla G., Cottin Y., Elbaz M., Coste P., Lemesle G., Motreff P., Popovic B., Khalife K., et al. Acute Myocardial Infarction: Changes in Patient Characteristics, Management, and 6-Month Outcomes Over a Period of 20 Years in the FAST-MI Program (French Registry of Acute ST-Elevation or Non-ST-Elevation Myocardial Infarction) 1995 to 2015. Circulation. 2017;136:1908–1919. doi: 10.1161/CIRCULATIONAHA.117.030798. - DOI - PubMed
-
- Degano I.R., Salomaa V., Veronesi G., Ferrieres J., Kirchberger I., Laks T., Havulinna A.S., Ruidavets J.B., Ferrario M.M., Meisinger C., et al. Twenty-five-year trends in myocardial infarction attack and mortality rates, and case-fatality, in six European populations. Heart. 2015;101:1413–1421. doi: 10.1136/heartjnl-2014-307310. - DOI - PubMed
-
- Schmidt M., Jacobsen J.B., Lash T.L., Botker H.E., Sorensen H.T. 25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: A Danish nationwide cohort study. BMJ. 2012;344:e356. doi: 10.1136/bmj.e356. - DOI - PMC - PubMed
-
- Cui Y., Hao K., Takahashi J., Miyata S., Shindo T., Nishimiya K., Kikuchi Y., Tsuburaya R., Matsumoto Y., Ito K., et al. Age-Specific Trends in the Incidence and In-Hospital Mortality of Acute Myocardial Infarction Over 30 Years in Japan- Report from the Miyagi AMI Registry Study. Circ. J. Off. J. Jpn. Circ. Soc. 2017;81:520–528. doi: 10.1253/circj.CJ-16-0799. - DOI - PubMed
LinkOut - more resources
Full Text Sources
