

Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in a central Chinese urban population: a cross-sectional survey
- PMID: 32245423
- PMCID: PMC7118942
- DOI: 10.1186/s12882-020-01761-5
Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in a central Chinese urban population: a cross-sectional survey
Abstract
Background: This study was conducted to evaluate and update the current prevalence of and risk factors for chronic kidney disease (CKD) and diabetic kidney disease (DKD) in a central Chinese urban population.
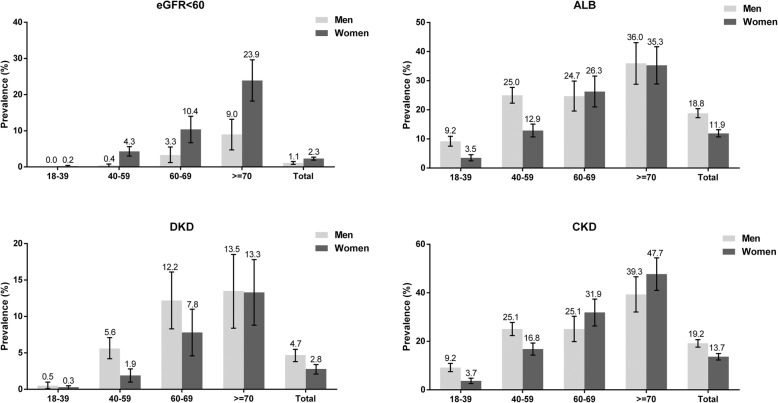
Methods: From December 2017 to June 2018, a total of 5231 subjects were randomly enrolled from 3 communities in 3 districts of Zhengzhou. CKD was defined as estimated glomerular filtration rate (eGFR) < 60 mL/min.1.73m2 or urinary albumin to creatinine ratio ≥ 30 mg/g (albuminuria). Diabetic subjects with systolic blood pressure > 140 mmHg, albuminuria or an eGFR less than 60 mL/min/1.73 m2 were classified as having DKD. Participants completed a questionnaire assessing lifestyle and relevant medical history, and blood and urine specimens were taken. Serum creatinine, uric acid, total cholesterol, triglycerides, low-density lipoprotein, high-density lipoprotein and urinary albumin were assessed. The age- and sex-adjusted prevalences of CKD and DKD were calculated, and risk factors associated with the presence of reduced eGFR, albuminuria, DKD, severity of albuminuria and progression of reduced renal function were analyzed by binary and ordinal logistic regression.
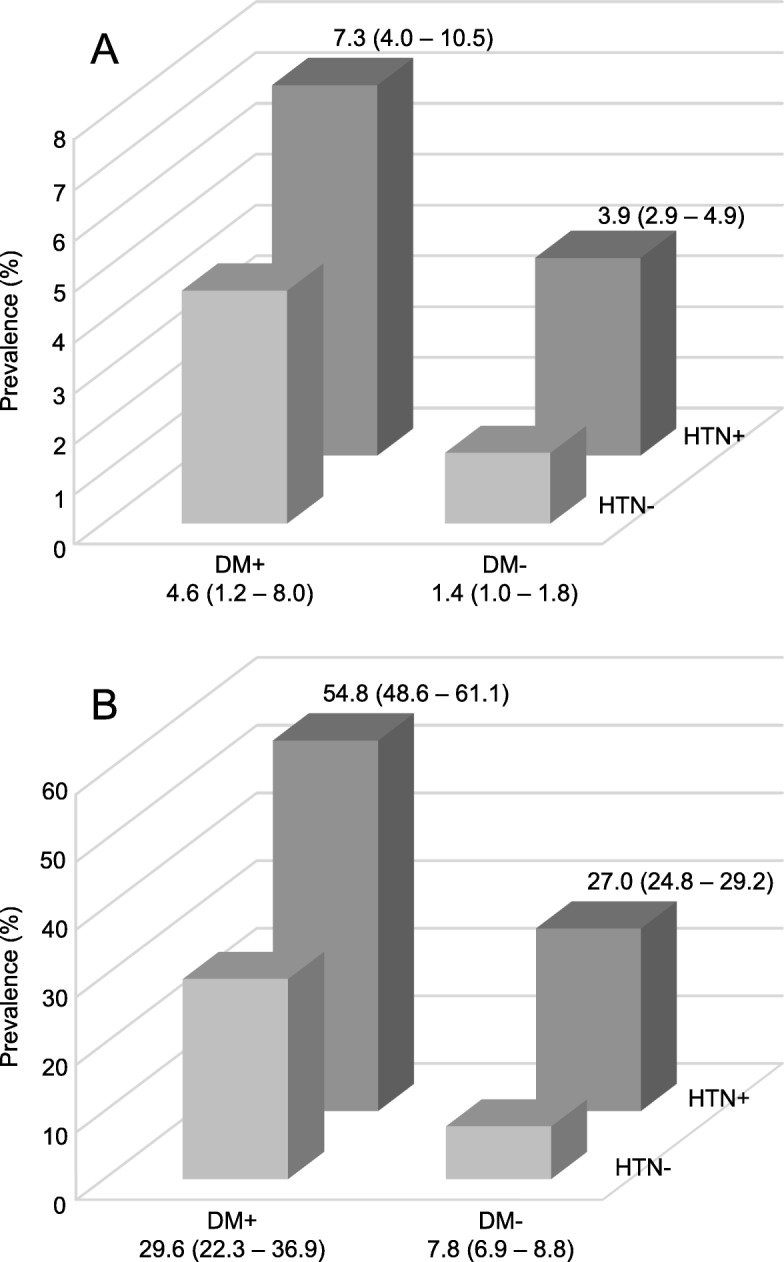
Results: The overall adjusted prevalence of CKD was 16.8% (15.8-17.8%) and that of DKD was 3.5% (3.0-4.0%). Decreased renal function was detected in 132 participants (2.9, 95% confidence interval [CI]: 2.5-3.2%), whereas albuminuria was found in 858 participants (14.9, 95% CI: 13.9-15.9%). In all participants with diabetes, the prevalence of reduced eGFR was 6.3% (95% CI = 3.9-8.6%) and that of albuminuria was 45.3% (95% CI = 40.4-50.1%). The overall prevalence of CKD in participants with diabetes was 48.0% (95% CI = 43.1-52.9%). The results of the binary and ordinal logistic regression indicated that the factors independently associated with a higher risk of reduced eGFR and albuminuria were older age, sex, smoking, alcohol consumption, overweight, obesity, diabetes, hypertension, dyslipidemia and hyperuricemia.
Conclusions: Our study shows the current prevalence of CKD and DKD in residents of Central China. The high prevalence suggests an urgent need to implement interventions to relieve the high burden of CKD and DKD in China.
Keywords: Chronic kidney disease; Diabetic kidney disease; Ordinal logistic regression; Prevalence.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Roth GA, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1736–1788. doi: 10.1016/S0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- Kyu HH, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1859–1922. doi: 10.1016/S0140-6736(18)32335-3. - DOI - PMC - PubMed
-
- Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1923–1994. doi: 10.1016/S0140-6736(18)32225-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
