

Routine diagnostics for neural antibodies, clinical correlates, treatment and functional outcome
- PMID: 32246252
- PMCID: PMC8213550
- DOI: 10.1007/s00415-020-09814-3
Routine diagnostics for neural antibodies, clinical correlates, treatment and functional outcome
Erratum in
-
Correction to: Routine diagnostics for neural antibodies, clinical correlates, treatment and functional outcome.J Neurol. 2020 Jul;267(7):2115-2116. doi: 10.1007/s00415-020-09855-8. J Neurol. 2020. PMID: 32399693 Free PMC article.
-
Correction to: Routine diagnostics for neural antibodies, clinical correlates, treatment and functional outcome.J Neurol. 2021 Aug;268(8):3056-3057. doi: 10.1007/s00415-021-10634-2. J Neurol. 2021. PMID: 34170405 Free PMC article. No abstract available.
Abstract
Objective: To determine frequencies, interlaboratory reproducibility, clinical ratings, and prognostic implications of neural antibodies in a routine laboratory setting in patients with suspected neuropsychiatric autoimmune conditions.
Methods: Earliest available samples from 10,919 patients were tested for a broad panel of neural antibodies. Sera that reacted with leucine-rich glioma-inactivated protein 1 (LGI1), contactin-associated protein-2 (CASPR2), or the voltage-gated potassium channel (VGKC) complex were retested for LGI1 and CASPR2 antibodies by another laboratory. Physicians in charge of patients with positive antibody results retrospectively reported on clinical, treatment, and outcome parameters.
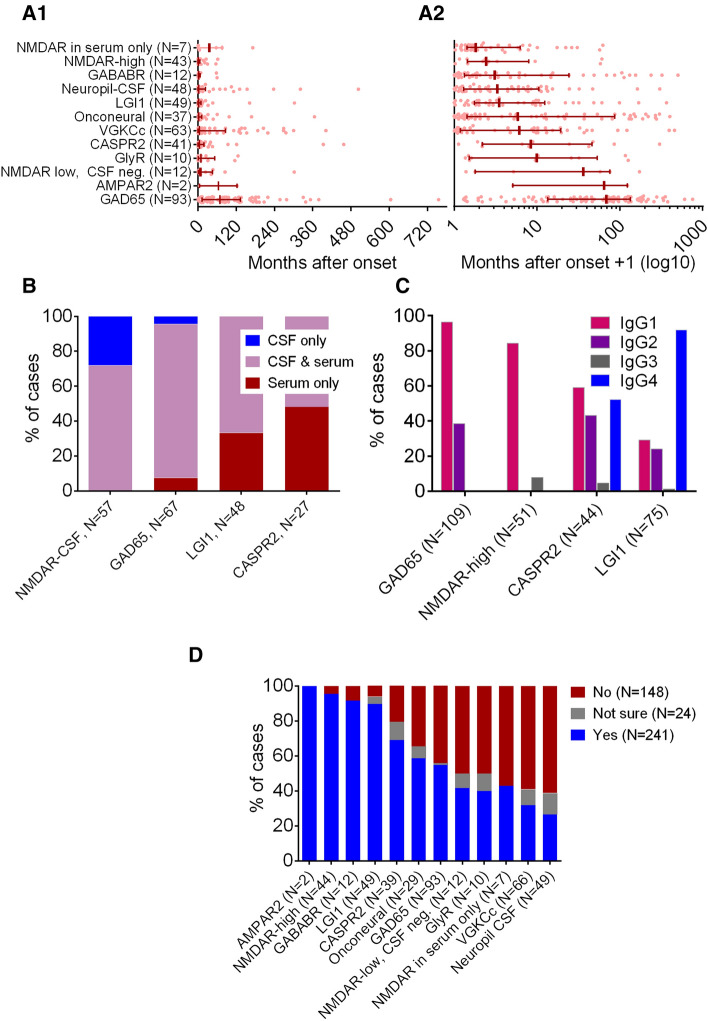
Results: Positive results were obtained for 576 patients (5.3%). Median disease duration was 6 months (interquartile range 0.6-46 months). In most patients, antibodies were detected both in CSF and serum. However, in 16 (28%) patients with N-methyl-D-aspartate receptor (NMDAR) antibodies, this diagnosis could be made only in cerebrospinal fluid (CSF). The two laboratories agreed largely on LGI1 and CASPR2 antibody diagnoses (κ = 0.95). The clinicians (413 responses, 71.7%) rated two-thirds of the antibody-positive patients as autoimmune. Antibodies against the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR), NMDAR (CSF or high serum titer), γ-aminobutyric acid-B receptor (GABABR), and LGI1 had ≥ 90% positive ratings, whereas antibodies against the glycine receptor, VGKC complex, or otherwise unspecified neuropil had ≤ 40% positive ratings. Of the patients with surface antibodies, 64% improved after ≥ 3 months, mostly with ≥ 1 immunotherapy intervention.
Conclusions: This novel approach starting from routine diagnostics in a dedicated laboratory provides reliable and useful results with therapeutic implications. Counseling should consider clinical presentation, demographic features, and antibody titers of the individual patient.
Keywords: Autoimmune encephalitis; Immunotherapy; Laboratory test evaluation; Neural autoantibodies; Outcome.
Conflict of interest statement
Dr. CG Bien obtained honoraria for speaking engagements from UCB, Desitin (Hamburg, Germany), and Euroimmun. He receives research support from Deutsche Forschungsgemeinschaft (German Research Council, Bonn, Germany) and Gerd-Altenhof-Stiftung (Deutsches Stiftungszentrum, Essen, Germany). Dr. M Holtkamp obtained speaker’s honoraria and/or consultancy fees from Arvelle, Bial, Desitin, Eisai, GW Pharmaceuticals, Novartis, and UCB. Dr. N Melzer has received honoraria for lecturing and travel expenses for attending meetings from Biogen Idec, GlaxoSmith Kline, Teva, Novartis Pharma, Bayer Healthcare, Genzyme, Alexion Pharmaceuticals, Fresenius Medical Care, Diamed, and BIAL, and has received financial research support from Euroimmun, Fresenius Medical Care, Diamed, Alexion Pharmaceuticals, and Novartis Pharma. Dr. F von Podewils obtained honoraria for speaking engagements from UCB, Eisai, and BIAL. Dr H Rauschka obtained honoraria for speaking engagements, consulting, serving on advisory boards and funding for conference travels from Biogen, Merck, Novartis, Roche, Sanofi and Teva-Ratiopharm. Dr. R Höftberger obtained honoraria for speaking engagements from Euroimmun and Novartis. She receives research support from the Jubiläumsfonds der Österreichischen Nationalbank, Project 16919, and the GBS/CIDP Foundation International. The Medical University of Vienna receives payments for antibody assays. The other authors report no conflicts of interest.
Figures


References
-
- Ariño H, Gresa-Arribas N, Blanco Y, Martinez-Hernandez E, Sabater L, Petit-Pedrol M, Rouco I, Bataller L, Dalmau JO, Saiz A, Graus F. Cerebellar ataxia and glutamic acid decarboxylase antibodies: immunologic profile and long-term effect of immunotherapy. JAMA Neurol. 2014;71:1009–1016. - PMC - PubMed
-
- Bien CG. Diagnosing autoimmune encephalitis based on clinical features and autoantibody findings. Expert Rev Clin Immunol. 2019;15:511–527. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
