

EAT-10 Scores and Fiberoptic Endoscopic Evaluation of Swallowing in Head and Neck Cancer Patients
- PMID: 32246779
- PMCID: PMC7754346
- DOI: 10.1002/lary.28626
EAT-10 Scores and Fiberoptic Endoscopic Evaluation of Swallowing in Head and Neck Cancer Patients
Abstract
Objective: The purpose of this study was to determine the relationship between patient-reported symptoms of oropharyngeal dysphagia (OD) using the Eating Assessment Tool (EAT)-10 and the swallowing function using a standardized fiberoptic endoscopic evaluation of swallowing (FEES) protocol in head and neck cancer (HNC) patients with confirmed OD.
Methods: Fifty-seven dysphagic HNC patients completed the EAT-10 and a FEES. Two blinded clinicians scored the randomized FEES examinations. Exclusion criteria consisted of presenting with a concurrent neurological disease, scoring below 23 on a Mini-Mental State Examination, being older than 85 years, having undergone a total laryngectomy, and being illiterate or blind. Descriptive statistics, linear regression, sensitivity, specificity, and predictive values were calculated.
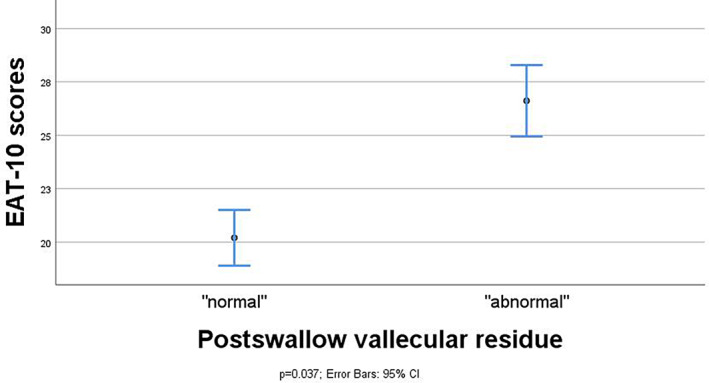
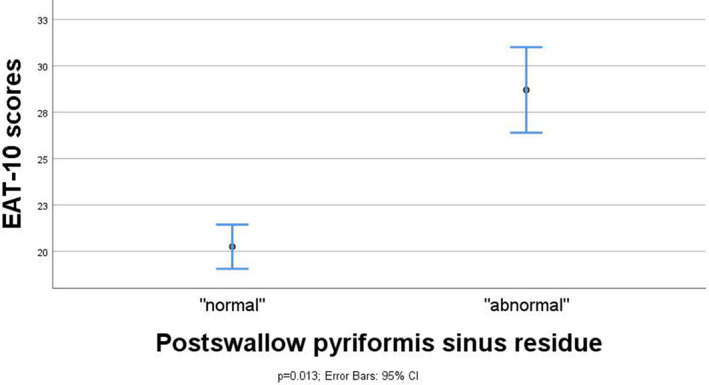
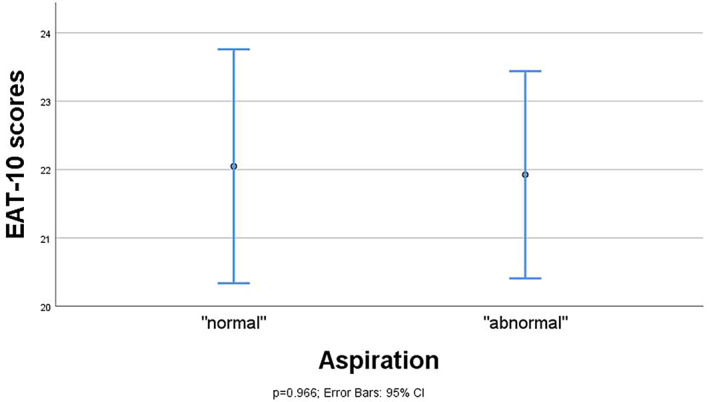
Results: The majority of the dysphagic patients (N = 38; 66.7%) aspirated after swallowing thin liquid consistency. A large number of patients showed postswallow pharyngeal residue while swallowing thick liquid consistency. More specifically, 42 (73.0%) patients presented postswallow vallecular residue, and 39 (67.9%) patients presented postswallow pyriform sinus residue. All dysphagic patients had an EAT-10 score ≥ 3. Linear regression analyses showed significant differences in mean EAT-10 scores between the dichotomized categories (abnormal vs. normal) of postswallow vallecular (P = .037) and pyriform sinus residue (P = .013). No statistically significant difference in mean EAT-10 scores between the dichotomized categories of penetration or aspiration was found (P = .966).
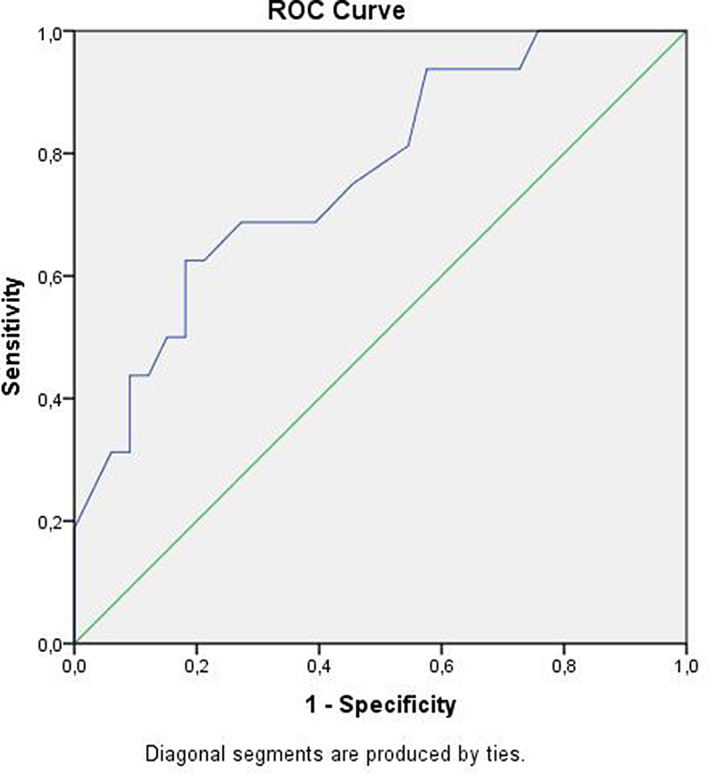
Conclusion: The EAT-10 questionnaire seems to have an indicative value for the presence of postswallow pharyngeal residue in dysphagic HNC patients, and a value of 19 points turned out to be useful as a cutoff point for the presence of pharyngeal residue in this study population.
Level of evidence: 2B.
Keywords: Dysphagia, deglutition, deglutition disorders, EAT-10, head and neck cancer.
© 2020 The Authors. The Laryngoscope published by Wiley Periodicals, Inc. on behalf of The American Laryngological, Rhinological and Otological Society, Inc.
Figures
References
-
- Mosel DD, Bauer RL, Lynch DP, Hwang ST. Oral complications in the treatment of cancer patients. Oral Dis 2011;17:550–559. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
