

The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017
- PMID: 32246941
- PMCID: PMC7232026
- DOI: 10.1016/S2468-1253(20)30007-8
The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017
Abstract
Background: Oesophageal cancer is a common and often fatal cancer that has two main histological subtypes: oesophageal squamous cell carcinoma and oesophageal adenocarcinoma. Updated statistics on the incidence and mortality of oesophageal cancer, and on the disability-adjusted life-years (DALYs) caused by the disease, can assist policy makers in allocating resources for prevention, treatment, and care of oesophageal cancer. We report the latest estimates of these statistics for 195 countries and territories between 1990 and 2017, by age, sex, and Socio-demographic Index (SDI), using data from the Global Burden of Diseases, Injuries, and Risk Factors Study 2017 (GBD).
Methods: We used data from vital registration systems, vital registration-samples, verbal autopsy records, and cancer registries, combined with relevant modelling, to estimate the mortality, incidence, and burden of oesophageal cancer from 1990 to 2017. Mortality-to-incidence ratios (MIRs) were estimated and fed into a Cause of Death Ensemble model (CODEm) including risk factors. MIRs were used for mortality and non-fatal modelling. Estimates of DALYs attributable to the main risk factors of oesophageal cancer available in GBD were also calculated. The proportion of oesophageal squamous cell carcinoma to all oesophageal cancers was extracted by use of publicly available data, and its variation was examined against SDI, the Healthcare Access and Quality (HAQ) Index, and available risk factors in GBD that are specific for oesophageal squamous cell carcinoma (eg, unimproved water source and indoor air pollution) and for oesophageal adenocarcinoma (gastro-oesophageal reflux disease).
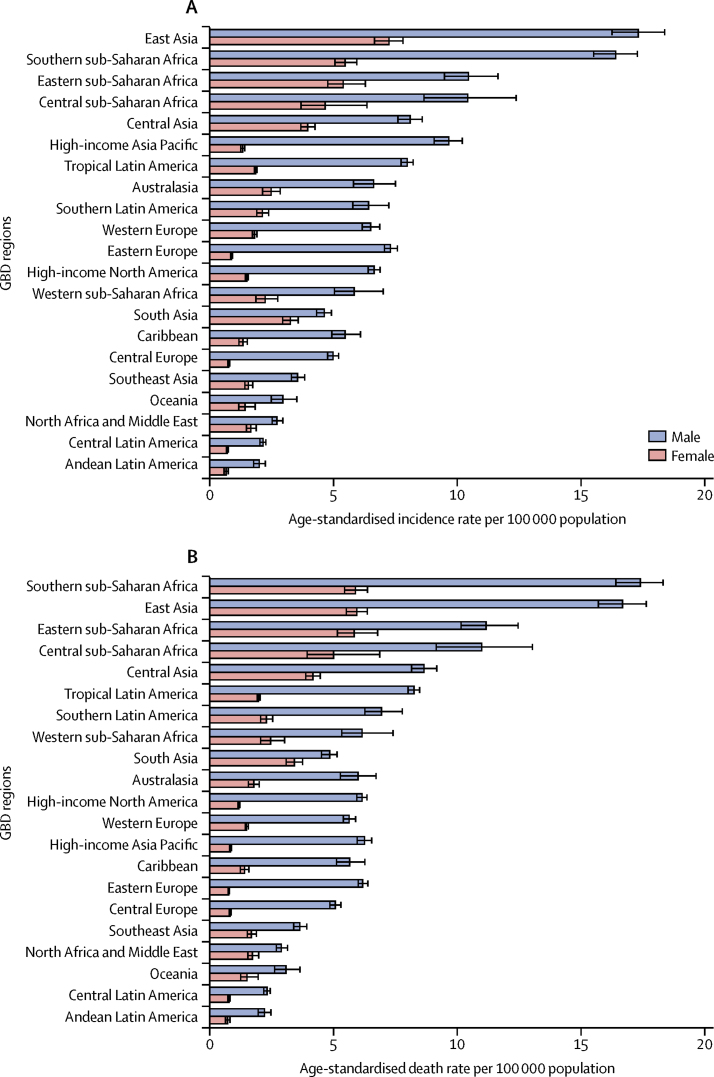
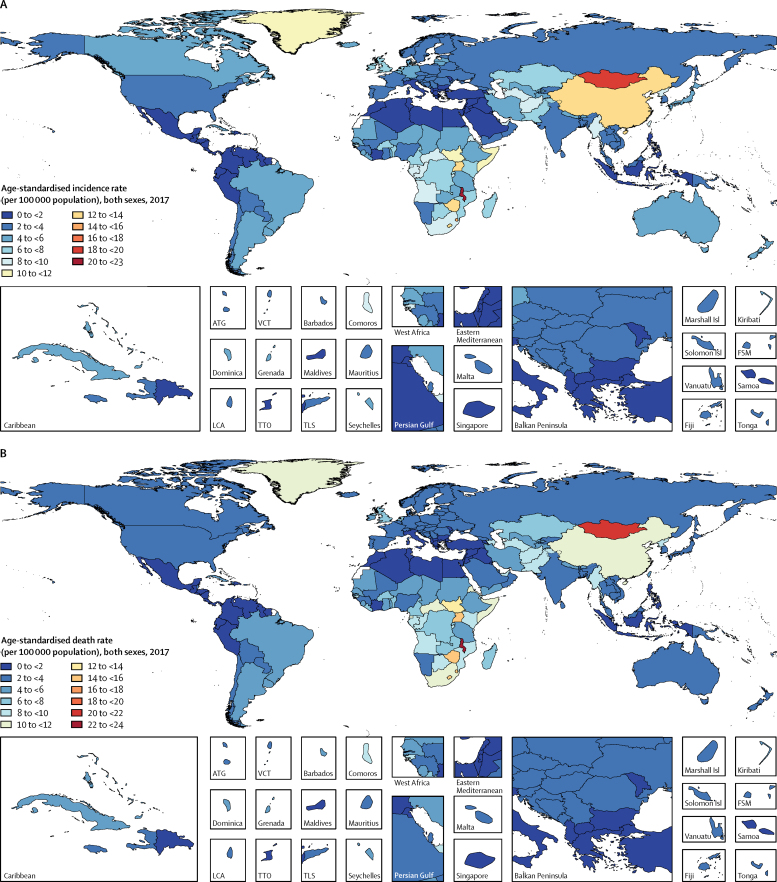
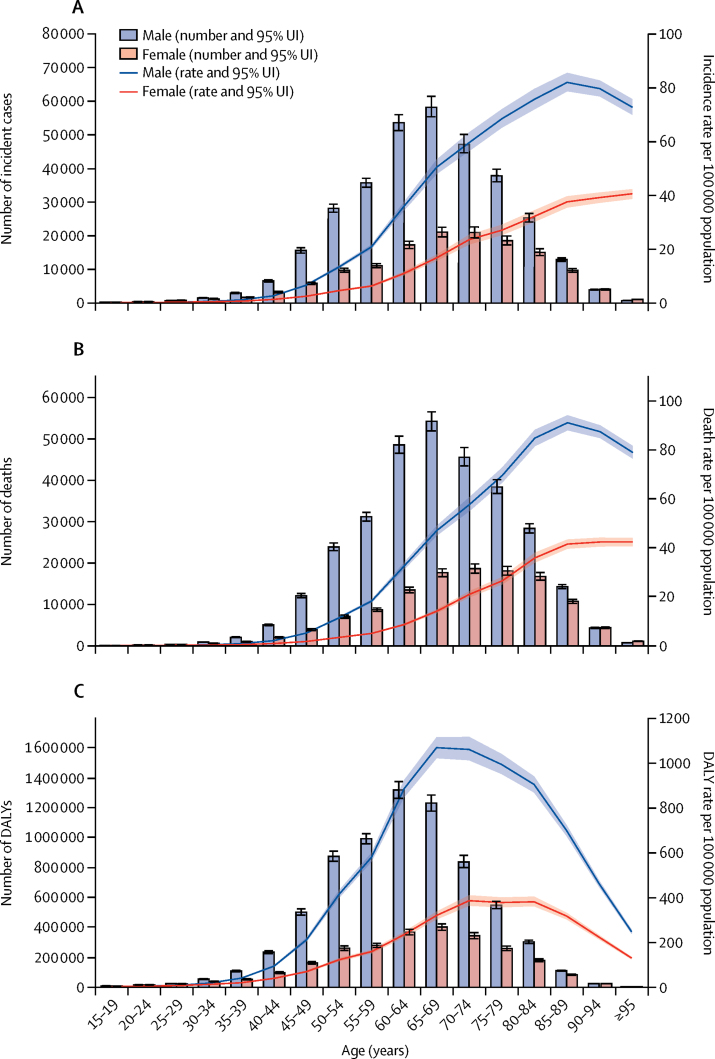
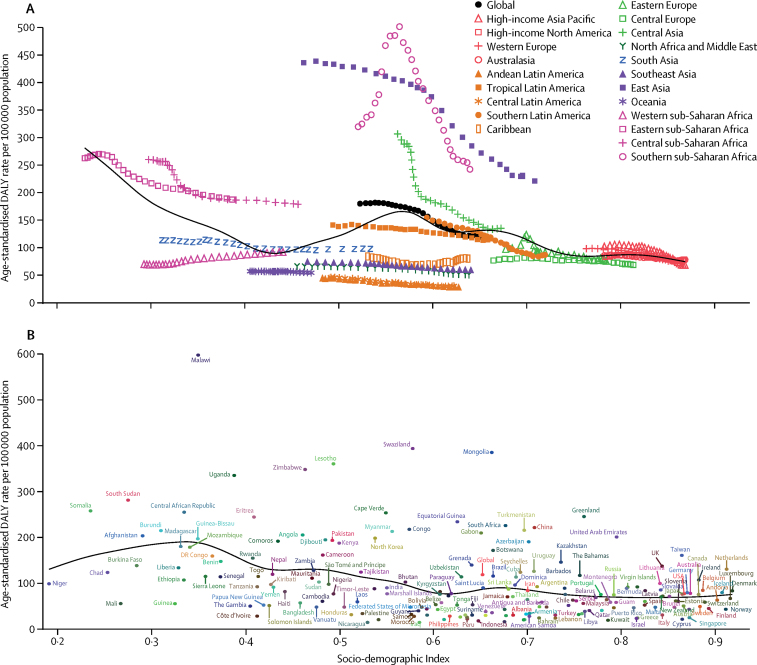
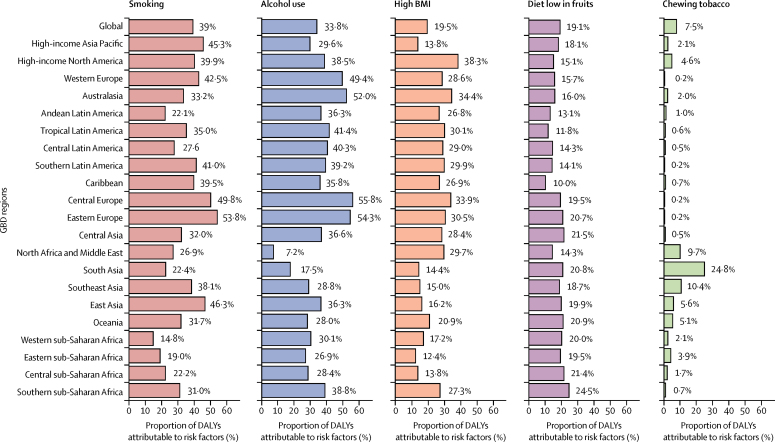
Findings: There were 473 000 (95% uncertainty interval [95% UI] 459 000-485 000) new cases of oesophageal cancer and 436 000 (425 000-448 000) deaths due to oesophageal cancer in 2017. Age-standardised incidence was 5·9 (5·7-6·1) per 100 000 population and age-standardised mortality was 5·5 (5·3-5·6) per 100 000. Oesophageal cancer caused 9·78 million (9·53-10·03) DALYs, with an age-standardised rate of 120 (117-123) per 100 000 population. Between 1990 and 2017, age-standardised incidence decreased by 22·0% (18·6-25·2), mortality decreased by 29·0% (25·8-32·0), and DALYs decreased by 33·4% (30·4-36·1) globally. However, as a result of population growth and ageing, the total number of new cases increased by 52·3% (45·9-58·9), from 310 000 (300 000-322 000) to 473 000 (459 000-485 000); the number of deaths increased by 40·0% (34·1-46·3), from 311 000 (301 000-323 000) to 436 000 (425 000-448 000); and total DALYs increased by 27·4% (22·1-33·1), from 7·68 million (7·42-7·97) to 9·78 million (9·53-10·03). At the national level, China had the highest number of incident cases (235 000 [223 000-246 000]), deaths (213 000 [203 000-223 000]), and DALYs (4·46 million [4·25-4·69]) in 2017. The highest national-level age-standardised incidence rates in 2017 were observed in Malawi (23·0 [19·4-26·5] per 100 000 population) and Mongolia (18·5 [16·4-20·8] per 100 000). In 2017, age-standardised incidence was 2·7 times higher, mortality 2·9 times higher, and DALYs 3·0 times higher in males than in females. In 2017, a substantial proportion of oesophageal cancer DALYs were attributable to known risk factors: tobacco smoking (39·0% [35·5-42·2]), alcohol consumption (33·8% [27·3-39·9]), high BMI (19·5% [6·3-36·0]), a diet low in fruits (19·1% [4·2-34·6]), and use of chewing tobacco (7·5% [5·2-9·6]). Countries with a low SDI and HAQ Index and high levels of indoor air pollution had a higher proportion of oesophageal squamous cell carcinoma to all oesophageal cancer cases than did countries with a high SDI and HAQ Index and with low levels of indoor air pollution.
Interpretation: Despite reductions in age-standardised incidence and mortality rates, oesophageal cancer remains a major cause of cancer mortality and burden across the world. Oesophageal cancer is a highly fatal disease, requiring increased primary prevention efforts and, possibly, screening in some high-risk areas. Substantial variation exists in age-standardised incidence rates across regions and countries, for reasons that are unclear.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Global Burden of Disease Cancer Collaboration Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the Global Burden of Disease Study. JAMA Oncol. 2017;3:524–548. - PMC - PubMed
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Global Burden of Disease Cancer Collaboration Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: a systematic analysis for the global burden of disease study. JAMA Oncol. 2019;5:1749–1768. - PMC - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF., Jr Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–2053. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
