

Age-Related and Gender-Related Increases in Colorectal Cancer Mortality Rates in Brazil Between 1979 and 2015: Projections for Continuing Rises in Disease
- PMID: 32248507
- PMCID: PMC7900022
- DOI: 10.1007/s12029-020-00399-8
Age-Related and Gender-Related Increases in Colorectal Cancer Mortality Rates in Brazil Between 1979 and 2015: Projections for Continuing Rises in Disease
Abstract
Purpose: Brazil is the largest country in South America. Although a developing nation, birth rates have been decreasing in the last few decades, while its overall population is undergoing lifestyle changes and ageing significantly. Moreover, Brazil has had increasingly high mortality rates related to colorectal cancer (CRC). Herein, we investigated whether the Brazilian population is exhibiting increasing mortality rates related to colon cancer (CC) or rectal cancer (RC) in recent years.
Methods: We examined data from the Brazilian Federal Government from 1979 to 2015 to determine whether CRC mortality and the population ageing process may be associated.
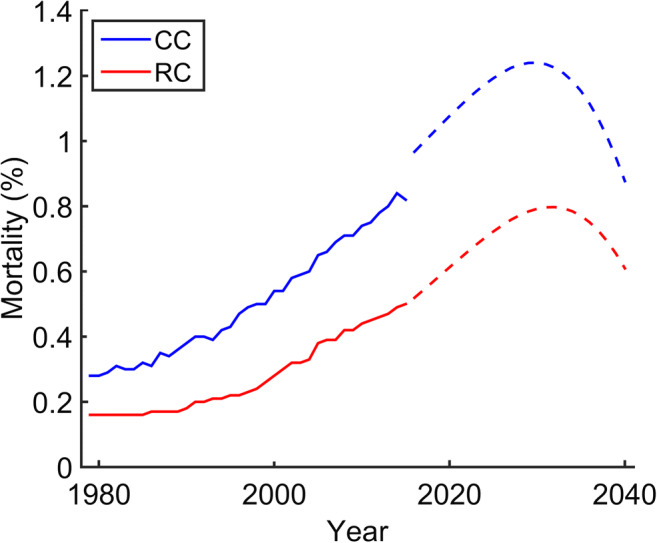
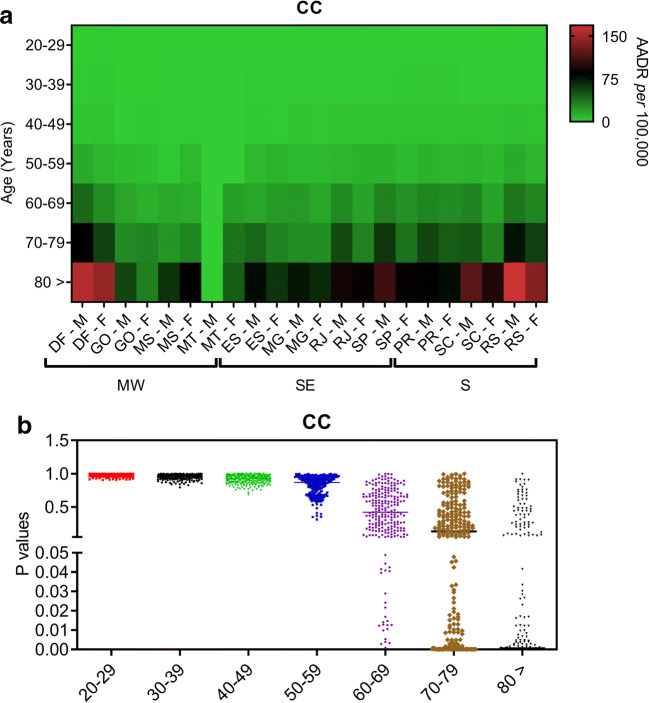
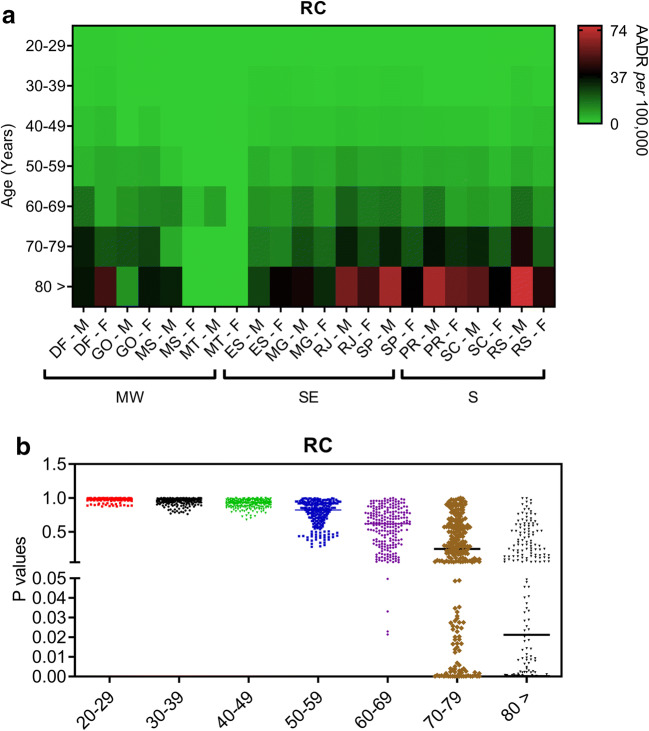
Results: Our mathematical modelling suggests that mortality rates related to CC and RC events in the Brazilian population may increase by 79% and 66% in the next 24 years, respectively. This finding led us to explore the mortality rates for both diseases in the country, and we observed that the highest levels were in the south and southeast regions from the year 2000 onwards. CC events appear to decrease life expectancy among people during their second decade of life in recent years, whereas RC events induced decreases in life expectancy in those aged >30 years. Additionally, both CC and RC events seem to promote significant mortality rates in the male population aged > 60 years and living in the southern states.
Conclusion: Our dataset suggests that both CC and RC events may lead to a significantly increasing number of deaths in the Brazilian male population in coming years.
Keywords: Ageing; Cancer mortality; Epidemiology; Lifestyle.
Conflict of interest statement
The authors declare that that they no competing interest.
Figures


Similar articles
-
Increasing crude and adjusted mortality rates for colorectal cancer in a developing South American country.Colorectal Dis. 2013 Jan;15(1):47-51. doi: 10.1111/j.1463-1318.2012.03110.x. Colorectal Dis. 2013. PMID: 22642835
-
[Colon and rectal cancer mortality in Brazilian capitals, 1980-1997].Arq Gastroenterol. 2005 Jan-Mar;42(1):63-70. doi: 10.1590/s0004-28032005000100014. Epub 2005 Jun 22. Arq Gastroenterol. 2005. PMID: 15976914 Portuguese.
-
Colorectal cancer mortality in Brazil: predictions until the year 2025 and cancer control implications.Dis Colon Rectum. 2014 Sep;57(9):1082-9. doi: 10.1097/DCR.0000000000000186. Dis Colon Rectum. 2014. PMID: 25101604
-
Incidence and mortality from colon and rectal cancer in Midwestern Brazil.Rev Bras Epidemiol. 2016 Oct-Dec;19(4):779-790. doi: 10.1590/1980-5497201600040008. Rev Bras Epidemiol. 2016. PMID: 28146167
-
Increased exposure to pesticides and colon cancer: Early evidence in Brazil.Chemosphere. 2018 Oct;209:623-631. doi: 10.1016/j.chemosphere.2018.06.118. Epub 2018 Jun 20. Chemosphere. 2018. PMID: 29957523
Cited by
-
A1, an innovative fluorinated CXCR4 inhibitor, redefines the therapeutic landscape in colorectal cancer.Cancer Cell Int. 2025 Jan 5;25(1):5. doi: 10.1186/s12935-024-03584-y. Cancer Cell Int. 2025. PMID: 39757159 Free PMC article.
-
Somatic targeted mutation profiling of colorectal cancer precursor lesions.BMC Med Genomics. 2022 Jun 28;15(1):143. doi: 10.1186/s12920-022-01294-w. BMC Med Genomics. 2022. PMID: 35761395 Free PMC article.
-
Geographic Distribution and Time Trends of Colorectal Cancer in Brazil from 2005 to 2018.Dig Dis Sci. 2022 Oct;67(10):4708-4718. doi: 10.1007/s10620-021-07357-9. Epub 2022 Jan 18. Dig Dis Sci. 2022. PMID: 35040020
References
-
- Sundling KE, Zhang R, Matkowskyj KA. Pathologic features of primary colon, rectal, and anal malignancies. Cancer Treat Res. 2016:168309–30. - PubMed
-
- Wang T, Maden SK, Luebeck GE, Li CI, Newcomb PA, Ulrich CM, Joo JE, Buchanan DD, Milne RL, Southey MC, Carter KT, Willbanks AR, Luo Y, Yu M, Grady WM. Dysfunctional epigenetic aging of the normal colon and colorectal cancer risk. Clin Epigenetics. 2020;12(1):5. doi: 10.1186/s13148-019-0801-3. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources