

Characterization of visceral leishmaniasis outbreak, Marsabit County, Kenya, 2014
- PMID: 32248804
- PMCID: PMC7132962
- DOI: 10.1186/s12889-020-08532-9
Characterization of visceral leishmaniasis outbreak, Marsabit County, Kenya, 2014
Abstract
Background: Visceral leishmaniasis (VL) is caused by protozoa of the Leishmania donovani complex. Annually, an estimated 500,000 cases of VL are reported globally posing a public health challenge. The objectives of our study were to confirm and determine the magnitude of VL outbreak, characterize the outbreak clinically and epidemiologically and evaluate the county preparedness and response in Marsabit County, Kenya.
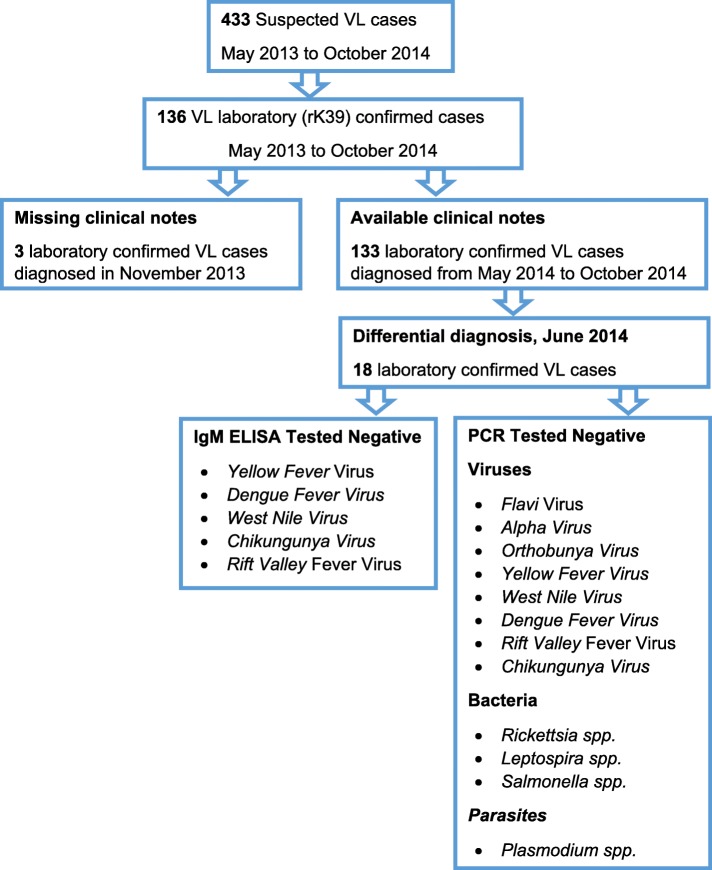
Methods: A retrospective review of laboratory registers and patients' clinical notes was done at Marsabit County Hospital. Cases were persons with confirmed VL diagnosis either by microscopy, serology or molecular technique coming from Marsabit County from May to October 2014. Cases were interviewed using structured questionnaire to collect clinical and epidemiologic information. Blood samples were collected from cases for laboratory confirmation.
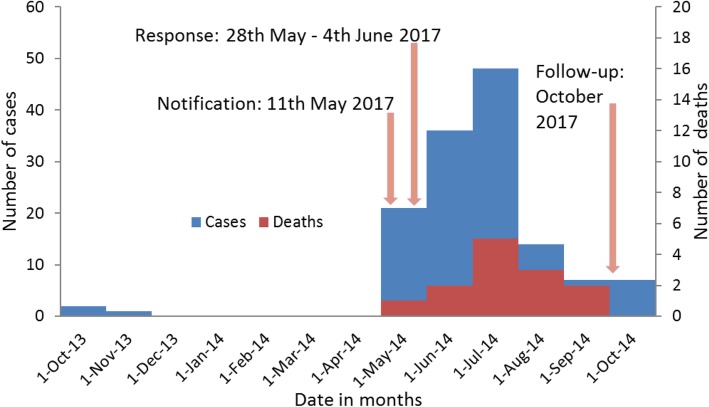
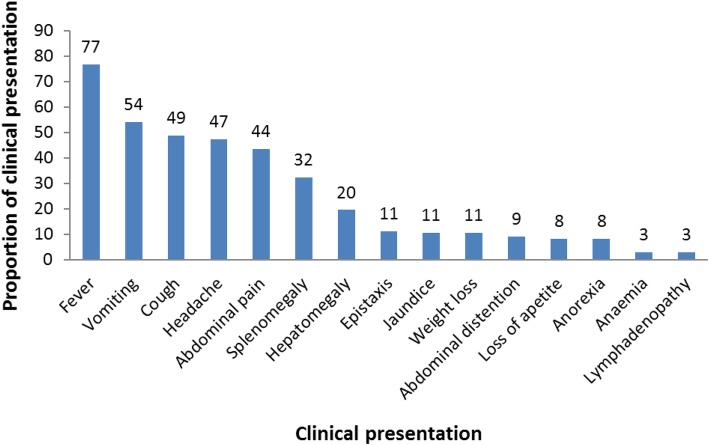
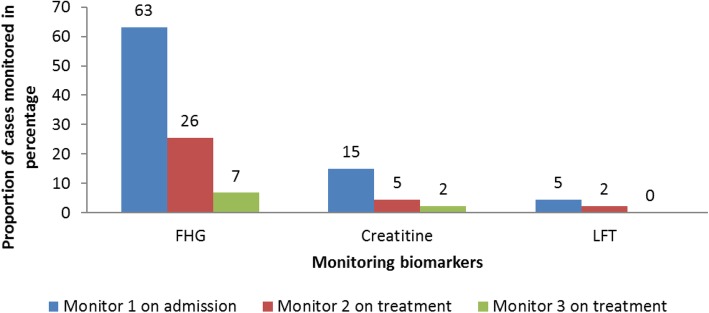
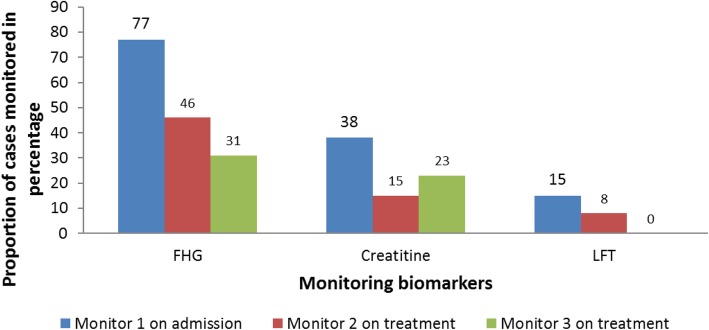
Results: A total of 136 cases were confirmed of which 77% (105) were male with a median age of 17 (IQR: 22) years and 9.6% (13) case fatality rate. All cases were admitted at Marsabit County Referral Hospital, Kenya. Medical records of 133 cases were retrieved. Of the 133 cases, 102 (77%) presented with fever, 43 (32%) with splenomegaly, 26 (20%) with hepatomegaly and 96 (72%) were managed with Sodium stibogluconate (SSG) monotherapy. Thirty-four cases (26%) received Full haemogram (FHG) test and none had more than one Liver Function Tests (LFTs) in a span of 6 months. Presenting with headache (OR: 4.21, 95% CI: 1.10-16.09) and hepatomegaly (OR: 4.2, 95% CI: 1.30-14.11) were associated with VL death. No VL case management training had been conducted nor VL treatment guidelines distributed among health care workers (HCWs) in the last 1 year.
Conclusions: VL cases were confirmed. Inadequate case monitoring and management was evident. VL case management sensitization training was conducted. The County health department should put in place one health VL surveillance and facilitate periodic case management trainings.
Keywords: Kala-azar; Kenya; Marsabit County; VL case management; Visceral leishmaniasis (VL).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ashford RW, Bettini S. The Leishmaniases in Biology and Medicine, Vol. 1. In: Peters W, Killick-Kendrick R, editors. Biology and Epidemiology. London: Academic Press; 1987. p. 550.
-
- Chappuis F, Mueller Y, Nguimfack A, Rwakimari JB, Couffignal S, Boelaert M, Cavailler P, Loutan L, Piola P. Diagnostic accuracy of two rK39 antigen-based dipsticks and the Formol gel test for the rapid diagnosis of visceral leishmaniasis in North-Eastern Uganda. J Clin Microbiol. 2005;43(12):5973–5977. doi: 10.1128/JCM.43.12.5973-5977.2005. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
