

Fetal antisense oligonucleotide therapy for congenital deafness and vestibular dysfunction
- PMID: 32249312
- PMCID: PMC7229850
- DOI: 10.1093/nar/gkaa194
Fetal antisense oligonucleotide therapy for congenital deafness and vestibular dysfunction
Abstract
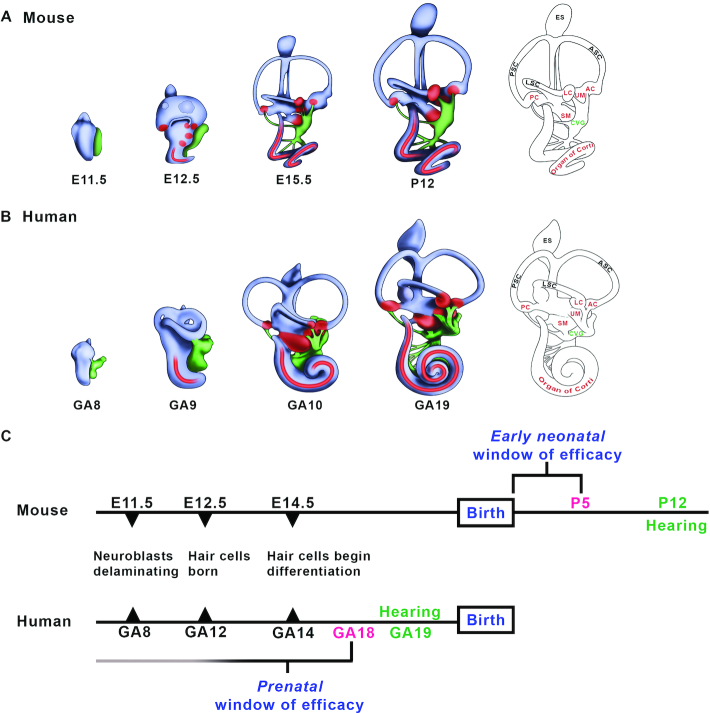
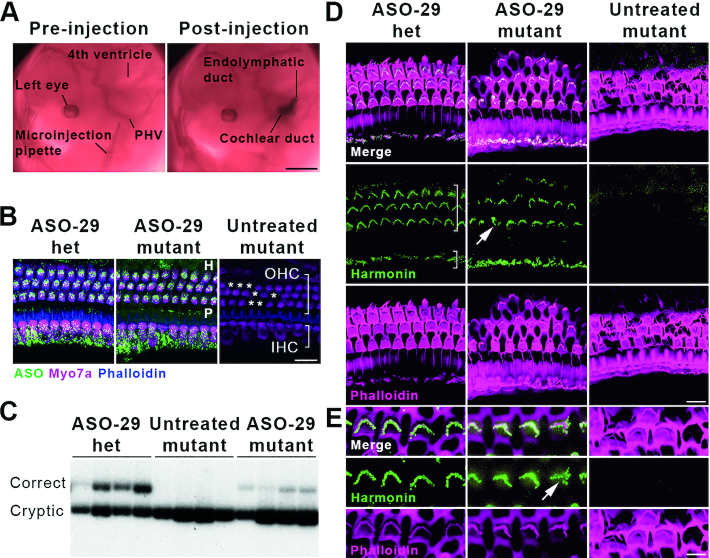
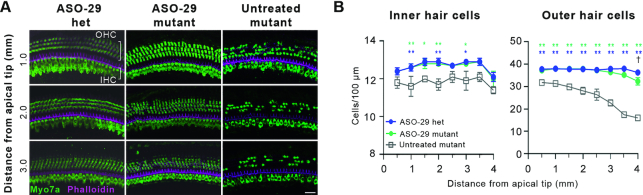
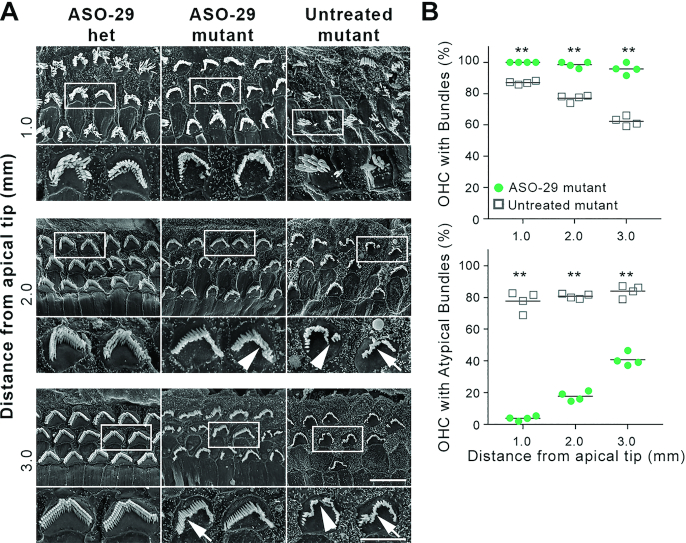
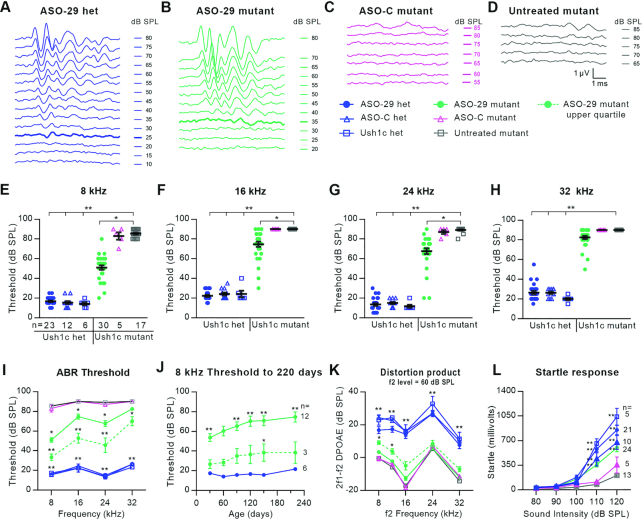
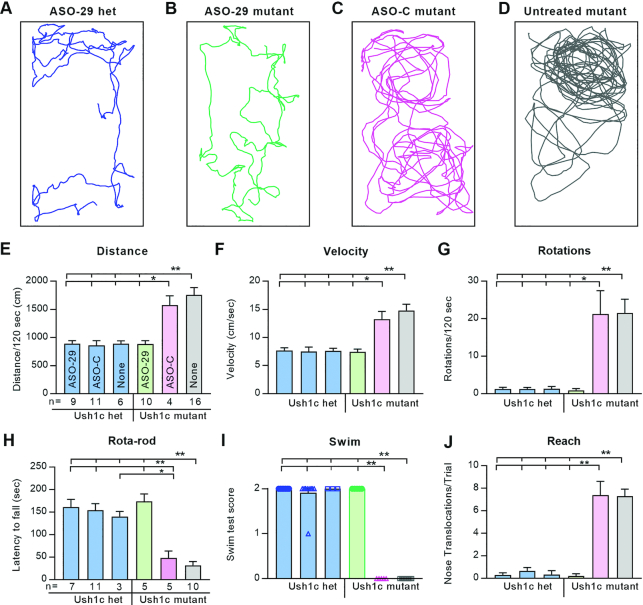
Disabling hearing loss impacts ∼466 million individuals worldwide with 34 million children affected. Gene and pharmacotherapeutic strategies to rescue auditory function in mouse models of human deafness are most effective when administered before hearing onset, after which therapeutic efficacy is significantly diminished or lost. We hypothesize that preemptive correction of a mutation in the fetal inner ear prior to maturation of the sensory epithelium will optimally restore sensory function. We previously demonstrated that transuterine microinjection of a splice-switching antisense oligonucleotide (ASO) into the amniotic cavity immediately surrounding the embryo on embryonic day 13-13.5 (E13-13.5) corrected pre-mRNA splicing in the juvenile Usher syndrome type 1c (Ush1c) mouse mutant. Here, we show that this strategy only marginally rescues hearing and partially rescues vestibular function. To improve therapeutic outcomes, we microinjected ASO directly into the E12.5 inner ear. A single intra-otic dose of ASO corrects harmonin RNA splicing, restores harmonin protein expression in sensory hair cell bundles, prevents hair cell loss, improves hearing sensitivity, and ameliorates vestibular dysfunction. Improvements in auditory and vestibular function were sustained well into adulthood. Our results demonstrate that an ASO pharmacotherapeutic administered to a developing organ system in utero preemptively corrects pre-mRNA splicing to abrogate the disease phenotype.
© The Author(s) 2020. Published by Oxford University Press on behalf of Nucleic Acids Research.
Figures
Similar articles
-
Direct Delivery of Antisense Oligonucleotides to the Middle and Inner Ear Improves Hearing and Balance in Usher Mice.Mol Ther. 2020 Dec 2;28(12):2662-2676. doi: 10.1016/j.ymthe.2020.08.002. Epub 2020 Aug 5. Mol Ther. 2020. PMID: 32818431 Free PMC article.
-
Rescue of hearing and vestibular function by antisense oligonucleotides in a mouse model of human deafness.Nat Med. 2013 Mar;19(3):345-50. doi: 10.1038/nm.3106. Epub 2013 Feb 4. Nat Med. 2013. PMID: 23380860 Free PMC article.
-
Rescue of Outer Hair Cells with Antisense Oligonucleotides in Usher Mice Is Dependent on Age of Treatment.J Assoc Res Otolaryngol. 2018 Feb;19(1):1-16. doi: 10.1007/s10162-017-0640-x. Epub 2017 Oct 12. J Assoc Res Otolaryngol. 2018. PMID: 29027038 Free PMC article.
-
Antisense Oligonucleotides for the Treatment of Inner Ear Dysfunction.Neurotherapeutics. 2019 Apr;16(2):348-359. doi: 10.1007/s13311-019-00729-0. Neurotherapeutics. 2019. PMID: 30972560 Free PMC article. Review.
-
Molecular basis of human Usher syndrome: deciphering the meshes of the Usher protein network provides insights into the pathomechanisms of the Usher disease.Exp Eye Res. 2006 Jul;83(1):97-119. doi: 10.1016/j.exer.2005.11.010. Epub 2006 Mar 20. Exp Eye Res. 2006. PMID: 16545802 Review.
Cited by
-
Recent Therapeutic Progress and Future Perspectives for the Treatment of Hearing Loss.Biomedicines. 2023 Dec 18;11(12):3347. doi: 10.3390/biomedicines11123347. Biomedicines. 2023. PMID: 38137568 Free PMC article. Review.
-
Usher Syndrome in the Inner Ear: Etiologies and Advances in Gene Therapy.Int J Mol Sci. 2021 Apr 10;22(8):3910. doi: 10.3390/ijms22083910. Int J Mol Sci. 2021. PMID: 33920085 Free PMC article. Review.
-
Current approaches for Usher syndrome disease models and developing therapies.Front Cell Dev Biol. 2025 Jun 20;13:1547523. doi: 10.3389/fcell.2025.1547523. eCollection 2025. Front Cell Dev Biol. 2025. PMID: 40620763 Free PMC article. Review.
-
Advances in gene therapy hold promise for treating hereditary hearing loss.Mol Ther. 2023 Apr 5;31(4):934-950. doi: 10.1016/j.ymthe.2023.02.001. Epub 2023 Feb 8. Mol Ther. 2023. PMID: 36755494 Free PMC article. Review.
-
Direct Delivery of Antisense Oligonucleotides to the Middle and Inner Ear Improves Hearing and Balance in Usher Mice.Mol Ther. 2020 Dec 2;28(12):2662-2676. doi: 10.1016/j.ymthe.2020.08.002. Epub 2020 Aug 5. Mol Ther. 2020. PMID: 32818431 Free PMC article.
References
-
- Olusanya B.O. Neonatal hearing screening and intervention in resource-limited settings: an overview. Arch. Dis. Child. 2012; 97:654–659. - PubMed
-
- Shearer A.E., Hildebrand M.S., Smith R.J.H.. Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Mefford HC, Stephens K, Amemiya A, Ledbetter N.. 1993; Seattle (WA)GeneReviews®.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
