

Multiple Respiratory Syncytial Virus Introductions Into a Neonatal Intensive Care Unit
- PMID: 32249314
- PMCID: PMC10936731
- DOI: 10.1093/jpids/piaa026
Multiple Respiratory Syncytial Virus Introductions Into a Neonatal Intensive Care Unit
Abstract
Background: Outbreaks of respiratory syncytial virus (RSV) in neonatal intensive care units (NICUs) are of concern because of the risk of severe disease in young infants. We describe an outbreak of RSV in a NICU and use whole genome sequencing (WGS) to better understand the relatedness of viruses among patients.
Methods: An investigation was conducted to identify patients and describe their clinical course. Infection control measures were implemented to prevent further spread. Respiratory specimens from outbreak-related patients and the community were tested using WGS. Phylogenetic trees were constructed to understand relatedness of the viruses.
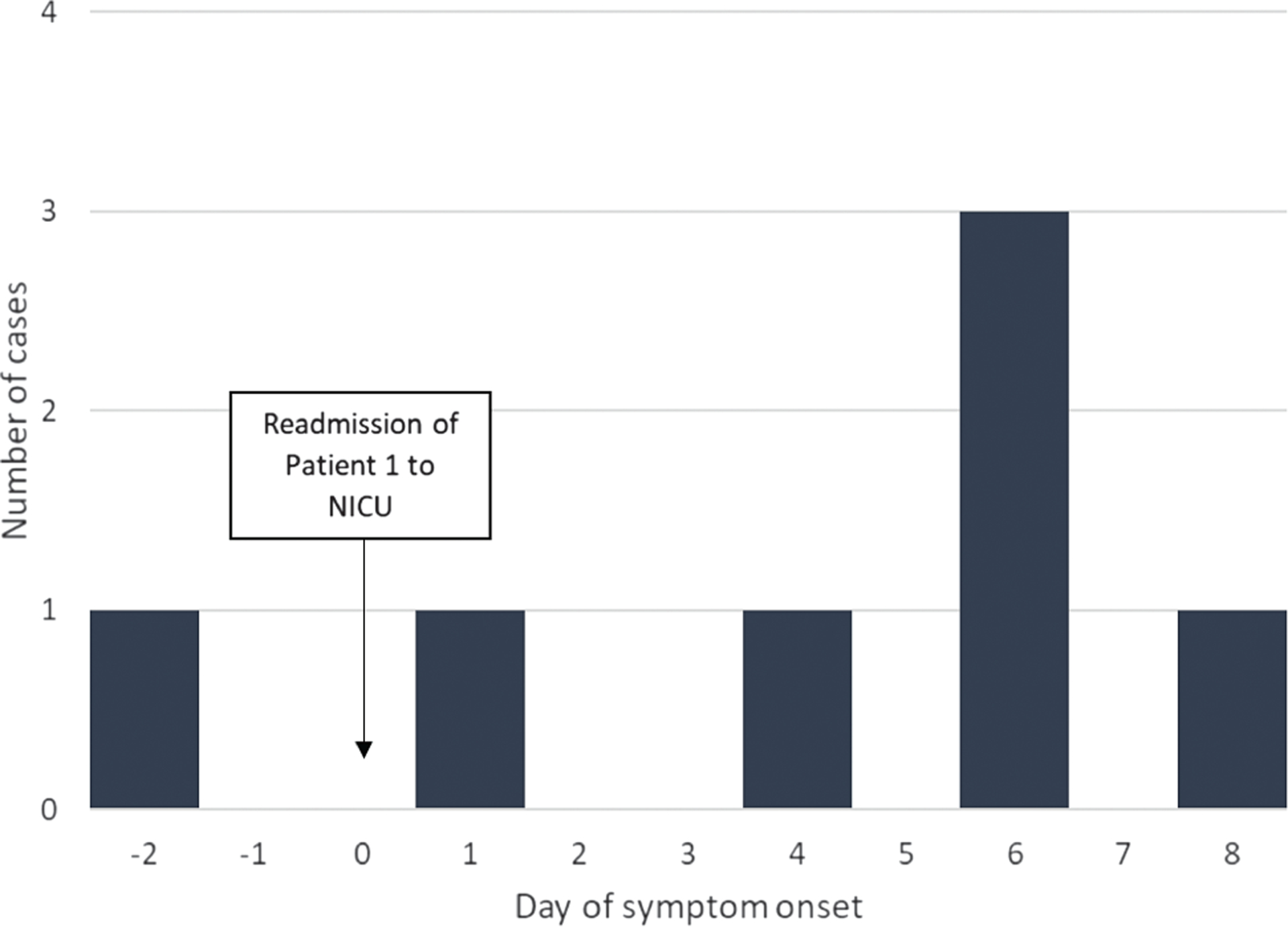
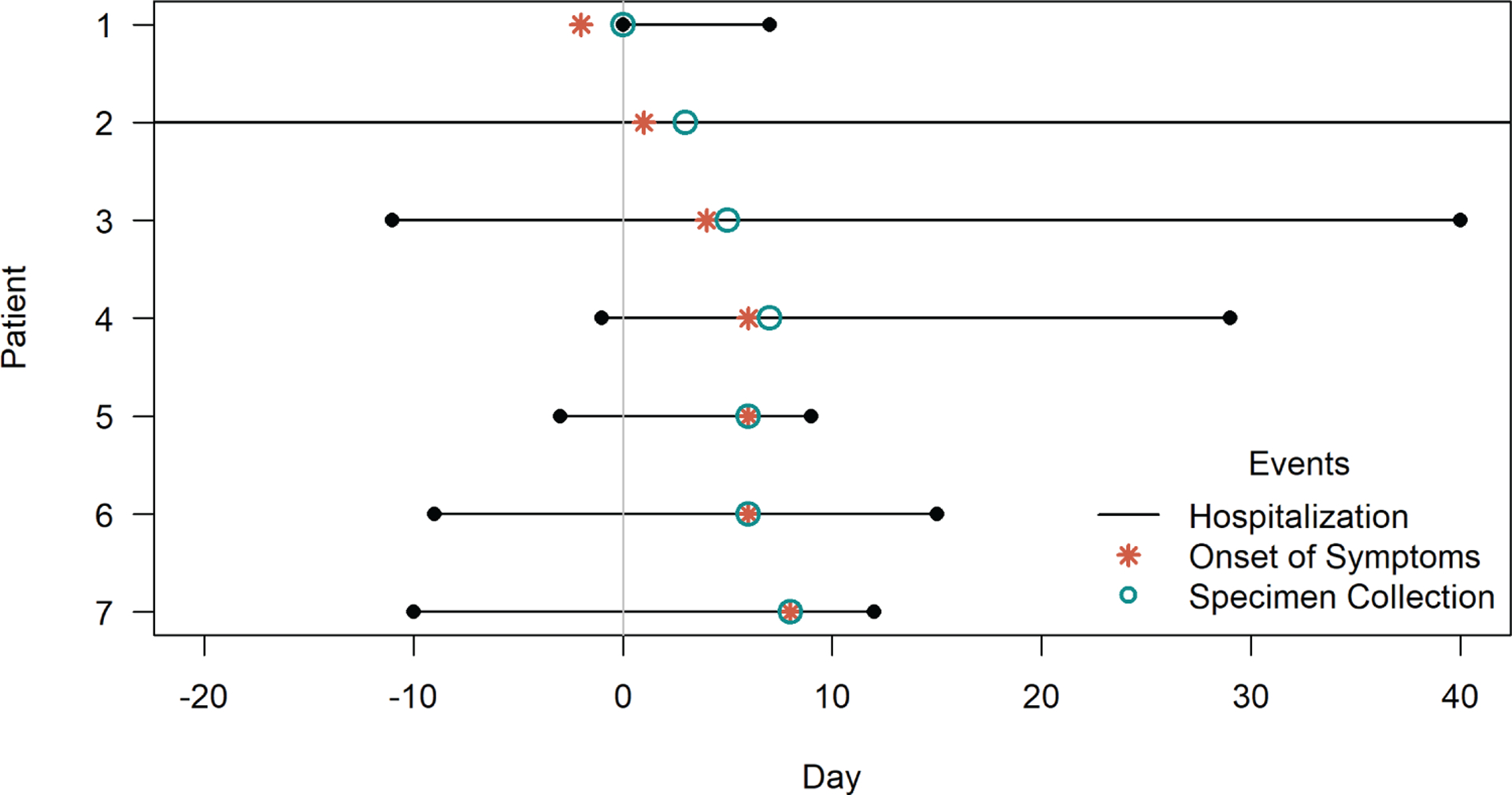
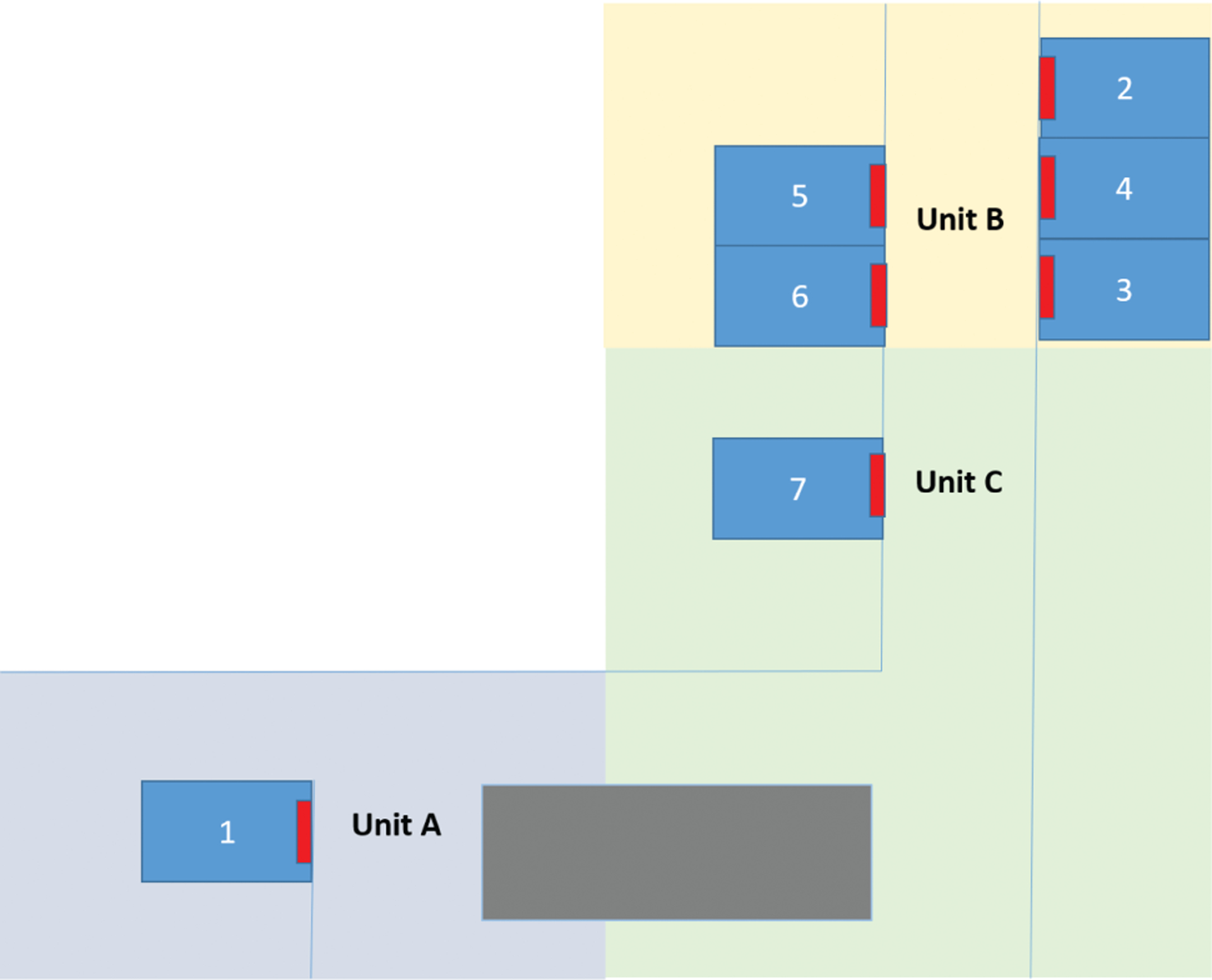
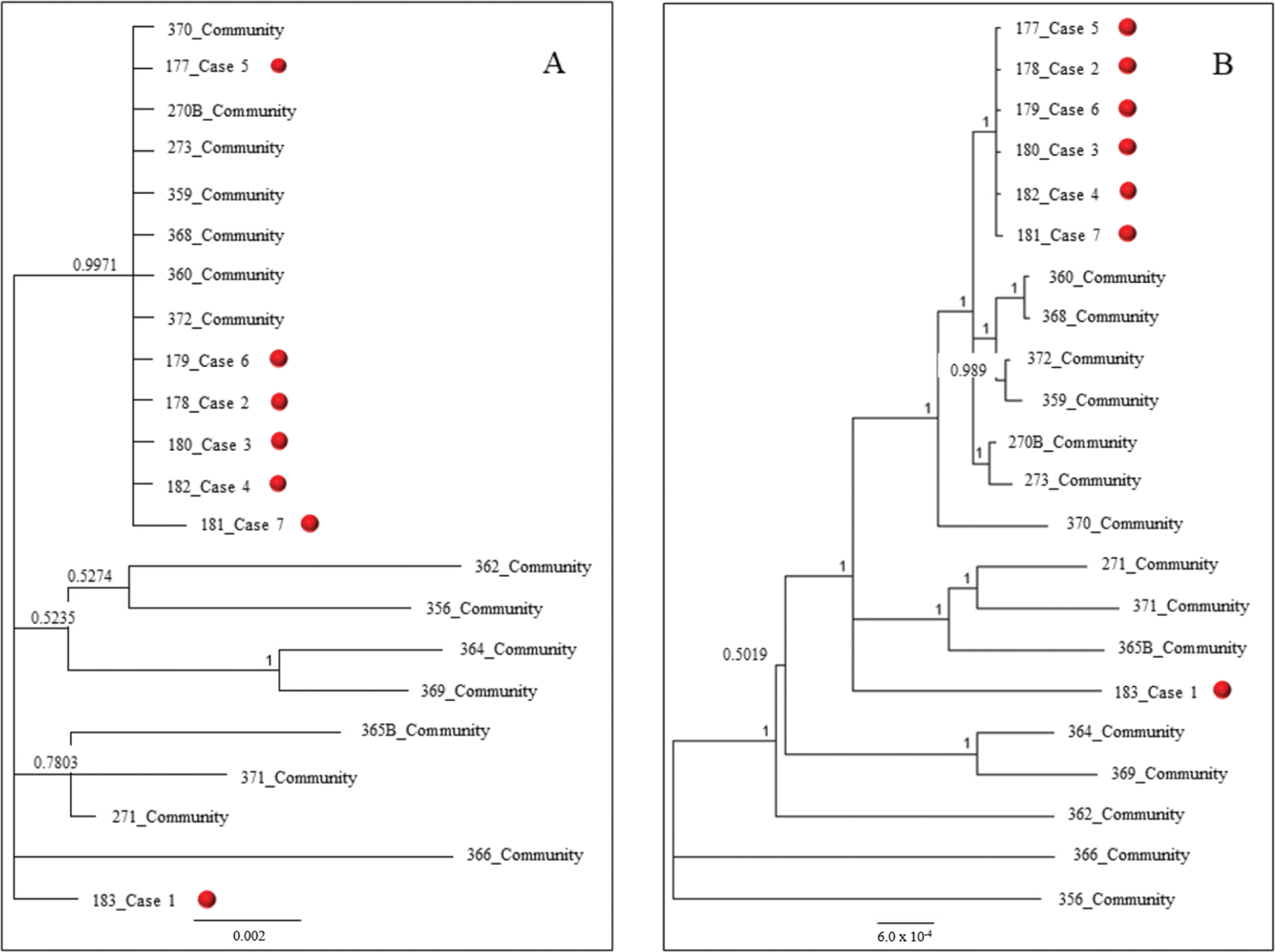
Results: Seven patients developed respiratory symptoms within an 11-day span in December 2017 and were diagnosed with RSV; 6 patients (86%) were preterm and 1 had chronic lung disease. Three patients required additional respiratory support after symptom onset, and none died. Six of 7 patients were part of the same cluster based on > 99.99% nucleotide agreement with each other and 3 unique single-nucleotide polymorphisms were identified in viruses sequenced from those patients. The seventh patient was admitted from the community with respiratory symptoms and had a genetically distinct virus that was not related to the other 6. Implementation of enhanced infection control measures likely limited the spread.
Conclusions: Using WGS, we found 2 distinct introductions of RSV into a NICU, highlighting the risk of healthcare-associated infections during RSV season. Early recognition and infection control measures likely limited spread, emphasizing the importance of considering RSV in the differential diagnosis of respiratory infections in healthcare settings.
Keywords: RSV; RSV outbreak; respiratory syncytial virus.
Published by Oxford University Press on behalf of The Journal of the Pediatric Infectious Diseases Society 2020.
Conflict of interest statement
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- American Academy of Pediatrics Committee on Infectious Diseases, American Academy of Pediatrics Bronchiolitis Guidelines Committee. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics 2014; 134:415–20. - PubMed
-
- Halasa NB, Williams JV, Wilson GJ, et al. Medical and economic impact of a respiratory syncytial virus outbreak in a neonatal intensive care unit. Pediatr Infect Dis J 2005; 24:1040–4. - PubMed
-
- Kilani RA. Respiratory syncytial virus (RSV) outbreak in the NICU: description of eight cases. J Trop Pediatr 2002; 48:118–22. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
